Download a pdf of this Memorandum
George W. Grayson is the Class of 1938 Professor of Government at the College of William & Mary, a board member of CIS, an associate scholar at FPRI, and a senior associate at the Center for Strategic & International Studies. His next book, Mexico: Narco-Violence and a Failed State? will be published this fall by Transaction Publishers.
The 24 members of the Congressional Hispanic Caucus (CHC) have voiced outrage that the pending health care reform will exclude illegal aliens. This prohibition may even spur the CHC and its allies in the House and Senate to shortchange their legal constituents by opposing HR 3200 or any related legislation that reaches the floor.
Even if the CHC hasn’t fathomed the public’s resentment to rewarding law-breakers, the message has reached the White House. President Barack Obama in his September speech to Congress on health care stopped talking about 47 million “people” who lack health insurance and began focusing on the 30 million “American citizens” who live without coverage.1 He went on to say that: “The reforms … I’m proposing would not apply to those who are here illegally,” a phrase that sparked Rep. Joe Wilson’s (R-S.C.) eruption: “You lie!” Sen. Max Baucus (D-Mont.) inscribed the chief executive’s pledge — along with a verification procedure — into the bill that was approved by the Senate Finance Committee on October 13.
The Hispanic Caucus, the National Council of La Raza, and other special pleaders are irate at the impact of Wilson’s fulmination. The outburst, said Rep. Luis V. Gutierrez (D-Ill.), an early Obama ally, was “said in a mean, ugly way. And what the president did was create an even meaner, uglier public policy to accompany it.” In the words of Brent A. Wilkes, national executive director of the League of United Latin American Citizens, the South Carolina legislator “acted like a buffoon, and everybody criticized him — but then at the end of the day he sort of got his way.”
This dissatisfaction over restrictions on illegal-alien access to taxpayer-funded health services was echoed at the Annual Binational Health Week events held in Santa Fe in early October. A report was released, produced jointly by the Mexican census agency CONAPO and the University of California, which lamented the lack of health coverage for the children of Mexican immigrants, much of it due to their or their parents’ illegal status.2 In reaction to the report, Mexico’s Interior Ministry said, “There is broad inequity in health services for minors under 18 in the United States.”3
These demands that American taxpayers subsidize the health care of Mexican immigrant families might be more persuasive were Mexico’s own health sector not in such desperate need of overhaul. Mexico’s health care system staggers under (1) grossly inadequate funding; (2) poor delivery of services; (3) a venal labor union, linked to job-selling and drug smuggling, that the chief executive’s National Action Party (PAN) has clasped to its bosom; and (4) fragmentation of government-subsidized providers.
This Memorandum will home in on the Mexican Social Security Institute (IMSS), which provides health and retirement benefits to 45.8 percent of the population. In addition, there is the modest Popular Health Insurance program or “Seguro Popular” (providing rudimentary assistance to the poorest quarter of the population), the Social Security and Services Institute for State Workers or ISSSTE (10.6 percent), and programs run by various states (1.3 percent). The Oil Workers’ Union, the two state electricity companies (CFE and LyFC),4 and the military (Social Security Institute of the Armed Forces, ISSFAM) have separate agencies (1.3 percent). Approximately 2.3 percent of the population relies on private insurance and the remaining 14.6 percent lack coverage. Many of these more than 15 million people live in rural, often indigenous communities. (The Organization of Economic Cooperation and Development (OECD) has found that 25 percent of the population lacks coverage.) Some of these individuals receive services from the Federal District and certain states have set up their own health and retirement schemes. President Felipe Calderón plans to extend Popular Security to those now left out in the cold.
Grossly Inadequate Funding
Although recent administrations have devoted more resources to health care in Mexico, the country still devotes only 6.1 percent of its gross domestic product to this crucial area — the lowest among the 30 members of the Paris-based OECD, with the exception of Turkey. It spends $523 per capita on health care each year compared with Turkey’s $615. In fact, Mexico’s per capita health expenditures are less than half what American taxpayers fork over to provide medical care for the two-thirds of all Mexican immigrants (nearly eight million people, legal and illegal) in the United States who are uninsured or on Medicaid.5

As a result, Mexico’s National Human Rights Commission (CNDH) has criticized the lack of general-practice physicians, specialists, and nurses, as well as “the insufficiency of beds, medicine, instruments, and medical equipment in general.”6 To make matters worse, administrative costs devour 10.8 percent of the nation’s health budget — more than twice the level for Medicare in the United States.7 In a country where red tape could be the national symbol, the multiple government-subsidized health care organizations and state-federal overlap of functions contribute greatly to delays, errors, and overhead expenses — a situation discussed below.
In addition, patients frequently complain about the arbitrary and capricious treatment received from IMSS personnel, who — thanks to union membership — have tenured positions.
Mexico falls at the bottom of the 30 OECD states in terms of out-of-pocket expenditures. The hemorrhaging of red ink has prompted its current director general, the well-regarded Daniel Karam, to ask Congress to dip into the IMSS’ 147,757,100 pesos ($11.4 billion) reserve fund to refurbish existing facilities, build new ones, purchase vitally needed equipment and medicines, and hire more professionals.8 Mexico’s social security system was designed for blue-collar workers; over the past decades, it has added peasants and poor people who qualify for Seguro Popular. Many of these new entrants pay extremely low premiums, if any, and the destitute are more likely to make greater demands on the plan. As in the United States, Mexico’s population is aging.
It is ironic that an ever-larger number of older Americans are going south of the border for such boutique health services as plastic surgery, knee replacements, and cosmetic dentistry. Needless to say, they patronize private practitioners, not public providers.
Fiscal reform to put social programs on a sound footing seems out of the question even though Mexico collects in taxes the equivalent of less than 12 percent of GDP, which puts it on a par with Haiti, a hopelessly failed state.
Poor Delivery of Services
A member of the business community recently gave insight into the quality of care provided by IMSS. In a letter to the newspaper Reforma, he wrote:
We own a restaurant with 98 employees. We pay each month an average of 180,000 pesos ($13,850) to IMSS. One of our workers, Érika Castro, who suffers severe heart ailments, has waited two months for an appointment with a cardiologist [even though] a general practitioner and another physician at the Cardiology Institute, to whom she went in desperation (and had to pay), told her that she required urgent care. She has complained to CONAMED (National Medical Arbitration Commission), which claimed they could do nothing. I regret to state for the umpteenth time that no one remembers why IMSS was established. The high dues are for professional and ethical attention to those who pay for service and not to inflate the salaries of indifferent and despotic doctors who believe that they are doing patients a favor to treat them.9
Physicians also complain about conditions. “The system is saturated, that’s the reality of it,” said Juan José González, the spokesman for the IMSS regional office in Guadalajara, Mexico’s second largest city. The overload is obvious at the IMSS Hospital No. 89 in Guadalajara, a well-worn facility where most American and other foreign retirees in the area go for major medical care. With just 226 beds, the 40-year-old hospital serves a potential clientele of 420,000 people referred by 60 clinics in Guadalajara and nearby towns and villages. The hospital’s emergency room team examines some 5,300 patients a month, many of whom are eventually admitted for extended care. But with beds in short supply, and three or four people to a room, patients often spend a restless night or two on gurneys in the halls of the emergency room. “This is our reality,” surgeon-administrator Salvador Orozco observed as he toured the emergency room while doctors and nurses scrambled to tend to more than 40 patients. “We do what we can,” Orozco said, “but we ask that the patients do what they can. Especially those who stay a long time.”10
It behooves a sick person to arrive at an IMSS clinic or hospital early to get a low-numbered slip (ficha); otherwise it is possible to wait for hours, and when the medical staff leaves, the individual must start again the next day. He has no choice of the doctor he sees. Depending upon the city or state, emergency operations may be scheduled promptly. Two- and three-month waits are the norm for non-critical procedures.
Lois Howland, a nursing teacher from San Diego, volunteered at an orphanage near Cuernavaca, a picturesque city south of the Federal District. Not only did she find the local health-care haphazard, she was taken aback by inadequate monitoring of treatment and follow-up exams. “You’re working with a country with limited resources,” she noted. “When I saw the Cuernavaca hospital, it looked like 1965.” There is a “huge disconnect, especially for indigenous people” to get access to decent medical care.11
“Mexicans will do almost anything to avoid a public hospital emergency room, where ailing patients may languish for hours slumped on cracked linoleum floors that smell of sweat, sickness, and pine-scented disinfectant. Many don’t see doctors at all, heading instead to the clerk at the corner pharmacy for advice on coping with a cold or a flu.”12
The OECD has pointed out that its affiliated countries have an average of 3.9 hospital beds for every 1,000 people. The IMSS figure is 0.83, which is down from 1.86 in 1980.13
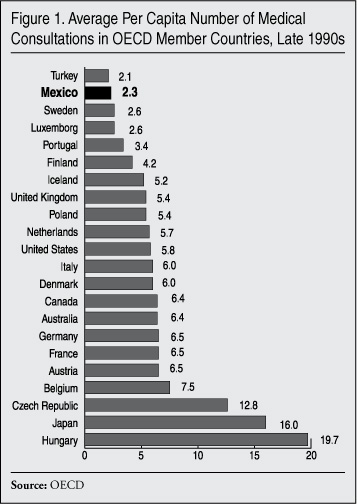
In view of population growth, the swine flu outbreak, and deteriorating incomes, it is reasonable to assume that the mean number of visits by Mexicans to medical professionals has declined since the OECD collected the data in Figure 1.
Venal Union
The Institutional Revolutionary Party (PRI), held the presidency from its founding in 1929 to the election of Vicente Fox, candidate of the center-right National Action Party (PAN), in 2000. Mexican chief executives cannot be reelected, and Felipe Calderón, also a PAN stalwart, succeeded Fox for the 2006-2012 term. A major key to the PRI’s seven-decade-long grip on power was “corporatism.” Taking a page from Italian dictator Benito Mussolini, large segments of the population were required to automatically affiliate with the so-called “revolutionary party” through trade unions, peasant leagues, and other employee groups.
Rather than power flowing from the bottom up, the corporatist PRI epitomized authoritarianism, paternalism, and coercion. For example, labor leaders were agents of the PRI establishment rather than representatives of their rank-and-file. Union honchos did the bidding of their superiors in the PRI-run government. In return for their loyalty, these chiefs, known as caciques, controlled hiring, manipulated internal elections, and obtained employment security, pay hikes, recreational facilities, and generous fringe benefits for members. For their part, union members backed the PRI with dues, votes, and attendance at rallies. Meanwhile, the caciques boasted opportunities to enrich themselves by selling tenured jobs, stealing material, forcing the public to pay bribes for services, and establishing their own “private” companies to sell goods and services to their employers at inflated prices.
The birth of IMSS in 1943 spawned one year later the creation of the National Union of Social Security Workers (SNTSS), which evinces the worst aspects of the corporatist regime. As Mexico moved toward greater transparency, the media began to report the shenanigans that suffused this union. An American labor report revealed that Eduardo “Lalo” Rodríguez López, the SNTSS’ general secretary, had engaged in “corrupt, gangster, anti-democratic acts, completely lacking in union ethics and consciousness ….” Leaders of Local 33, which embraces 23,000 workers from clinics and hospitals in the Mexico Valley, accused him of dispatching goons to seize their funds and destroy documents, while holding innocent bystanders captive.14 Rodríguez López was no stranger to the drug scene. In the mid-1990s, when he was secretary of the STNSS’ local 33, he was arrested in Mexico City’s Venustiano Carranza borough, presumably for drug possession.
Although political connections kept him out of prison, Rodríguez López reportedly continued his nefarious practices while a supervisor at the General Hospital of the Medical Center La Raza in Mexico City. This sprawling, labyrinthine facility employs 14,500 nurses, doctors, orderlies, and other personnel. On average, 50,000 workers, patients, and family members visit the La Raza each day.
Investigative journalists assert that Rodríguez López masterminded an elaborate scheme to illegally distribute drugs from the hospital. Before Mexico’s Attorney General Office (PGR) launched an investigation several years ago, the SNTSS stalwart allegedly protected his couriers with an elaborate system of lookouts, even as he intimidated authorities to keep them quiet. Not only were IMSS’ agents selling to outsiders, but professionals often worked while under the influence of drugs. In the words of one employee:
There are doctors that perform their duties while drugged, nurses who are tense as if under the influence of some stimulant. It is frequent to see people who, on the pretext of having an examination, enter into transactions: paying [for drugs], delivering drugs, or simply warning of some risk or danger that could affect the organization.15
Sales of drugs originating from La Raza were not limited to the domestic market. On September 14, 2005, Spanish police arrested Israel Gutiérrez Botello, a Mexican citizen who had ingested 70 capsules of cocaine. The 21-year-old, whose erratic behavior in the Madrid airport gave him away, was in Europe not only to market narcotics, but to collect payments.
Israel is the son of Valdemar Gutiérrez Fragoso, who enjoyed the backing of Rodríguez López and former SNTSS president Roberto Javier Vega Galina in attaining the union’s number-one spot on October 12, 2006. There was no secret ballot. After a show of hands, with opposition contenders repressed, the tequila and whiskey aficionado Gutiérrez Fragoso was declared the winner. Because of the chaos in the union election site, the new leader swore the oath of office in a ceremony that lasted no more than 25 seconds.16
His adversaries continue to pelt him with charges. In late 2008, at a Congress of Local 27 in Campeche, many of the 140 delegates joined in lambasting union leaders for selling jobs to prospective doctors and nurses in IMSS for 30,000 pesos ($2,300), enriching themselves with SNTSS funds, deriving monies from a restaurant-bar opened in a union building, and nepotism. The protesters claimed that two sons and a brother-in-law of the local’s leader got well-paid jobs for which they were not qualified. So explosive was the atmosphere that the besieged local chief fled through the back door at his earliest opportunity.17 Charges of nepotism have also haunted the leader of the SNTSS local in Ciudad Victoria, the capital of Tamaulipas state.18
Meanwhile, authorities have turned up black market dealing in corneas needed for transplants. These tissues were missing from the Ophthalmology Hospital of the National Medical Center Century XXI in Mexico City. While investigating the case, authorities found that an IMSS administrative director was the majority owner of a firm that sold medicines to the agency. They also found inadequate controls over the purchase of radioactive material.19
As a loyal vassal of the PRI, the SNTSS gained one benefit after another. Not only did union members boast tenured positions, relatively high salaries, free medical care, generous Christmas bonuses, and additional compensation for arriving at work on time, but their retirement plan was one of the most attractive in the country. The lion’s share of the nation’s 374,000 SNTSS members can retire with pensions in their middle 50s compared with the minimum retirement age of 65 for most other Mexicans. Women who work at IMSS can retire with full pensions after 27 years of service, regardless of age; men must work 28 years before they enjoy equal treatment. Not only do these pensions equal the highest salary earned by the worker before he or she retired, they also include raises received by current employees, as well as free medical care for the pensioner.
Some 120,000 doctors, nurses, orderlies, and staff members receive these benefits, even if — in the case of a physician or nurse practitioner — he or she opens a private practice or continues in the private clinic at which he or she supplemented his or her income when employed by IMSS. Even without a second job, a doctor retired from IMSS receives 17.3 percent more income than when he or she was employed; a nurse receives 26.7 percent more; and an orderly 33.3 percent more.20
Both IMSS and the SNTSS keep a lid on the details of the collective contract signed every two years between the entities. However, an intrepid reporter published some of the elements of the 2006 agreement. In this accord, the government in 2006 earmarked 14,238,000 ($1.3 million) to cover the salaries of union leaders, as well as the pay provided to IMSS staff members who handle the workers’ benefits. Moreover, IMSS earmarked 415,291,200 pesos ($38.5 million) for new vehicles for union leaders. In addition, money was allocated for housing loans (787,543,200 pesos/$72.9 million), legal matters (41,438,400 pesos/$3.8 million), scholarships (688 million pesos/$63 million), and tax obligations of SNTSS members (6,842,016,981 pesos/$633.5 million).21 It did not include, however, a rumored perk included in the SME electricians’ union pact, which reportedly allows members suffering stress to swim with dolphins in Cancún on the government’s tab. Despite these outlays, the union keeps information about its members under wraps.
A 2008 reform increased to 34 (women) and 35 (men) the years they must work before receiving full pensions and raised the retirement age to 60. Still, these provisions apply only to the newly hired — that is, 54,212 of IMSS’ 379,106 workers.22
No wonder Mexico City pundits joke that: “Young people don’t study to become doctors or nurses, they train to become pensioners.”
Felipe Calderón’s National Action Party has railed against corruption arising from the PRI’s corporatist practices. Upon swearing the oath of office in 2006, the new chief executive committed himself to this goal. Instead of battling the boss-ridden unions and the bloated workforces they have spawned, he has cut deals with the obscenely corrupt Oil Workers’ Union and the SNTE Teachers’ Union. The latter, which has colonized public education in the country, is led by Elba Esther Gordillo Morales.23
Valdemar Gutiérrez Fragoso is a political chameleon par excellence. He backed messianic populist Andrés Manuel López Obrador, candidate of the leftist Democratic Revolutionary Party in 2006; he next reached an agreement with the PRI to run on its ticket in 2009. Not only has the National Action Party failed to cross swords with Valdemar Gutiérrez Fragoso, it outbid the PRI in order to ensure the 49-year-old smarmy boss a safe seat in the Chamber of Deputies.24 The PAN’s erstwhile president justified this move because: “National Action respects the autonomy of organized labor and the democratic and plural political participation of union members in Mexico.”25
It would be nice if the incorporation of a leading health official into the PAN meant that the sector was going to suddenly get more attention. As recent reports triggered by the swine flu outbreak have demonstrated, however, the Mexican health system remains severely fragmented, under-staffed, under-resourced, and burdened by high absenteeism among physicians. Fixing it requires more money, but also new and improved labor relations and a new professionalism on the part of health workers.26
Fragmentation
As indicated earlier, the Mexican government finances a half-dozen or so separate health care and pension systems. This crazy-quilt arrangement guarantees waste, redundancy of services, and loss of economies of scale.
Traditionally, IMSS participants were expected to seek service at the clinics and hospitals closest to their homes. Needless to say, such a rule left a resident of Mexico City in a Catch 22 situation should he become ill in Oaxaca. IMSS has moved toward providing treatment to its clients regardless of where their need arises.
The greater problem lies in the difficulty — sometimes the inability — of an IMSS card-holder to obtain medical care at a facility operated by ISSSTE, Pemex, the armed forces, or other agencies. Only in a dire emergency is an ISSFAM health care professional likely to render service to a civilian who does not belong to a military family. Pemex, which prides itself on excellent care for oil workers, is also reluctant to render attention to non-petroleros or their family members.
Even though President Calderón earned plaudits for handling the spring 2009 swine flu epidemic, the PRI-fashioned health care sector drew scorn from doctors and nurses as weak, obsolete, and fragmented. Among other gross deficiencies, the half-dozen or more public systems have different databases, which delay ascertaining the characteristics, nature, and scope of a disease.27
Mexico’s metropolitan areas boast state-of-the-art hospitals stocked with modern equipment and staffed by U.S. board-certified specialists. As previously mentioned, more and more Americans take advantage of world-class care at low costs in these facilities. IMSS and ISSSTE hospitals represent another world. “Some patients suspected of having swine flu told the Associated Press that public hospitals turned them away or forced them to wait for hours for treatment even after the government declared a national emergency.”28
A fractured system may have led to multiple deaths in a fire at an IMSS-licensed day-care facility in northern Sonora state in mid-2009. The institute has responsibility for granting the right to operate to one network of facilities, and the Social Development Ministry grants concessions for another network. The National Human Rights Commission found that the ABC center where 49 youngsters perished was too small for the number of children enrolled, lacked proper ventilation, and failed to meet safety standards. Who was to blame? The CNDH pointed its finger at IMSS and the state and local government. Nevertheless, it seemed to be a case of “everyone was in charge and no one was in charge.”29
Conclusion
Even as their advocates lobby fiercely for the coverage of illegal aliens under any health care initiative that emerges from the U.S. Congress, Mexico struggles under an unwieldy, fragmented, corrupt, and inefficient system, with the result that their citizens who come to this country legally or illegally often place a disproportionate burden on U.S. taxpayers. Emigration itself may be more attractive because of Mexico’s neglect of its health sector. As stated earlier, American taxpayers annually provide more than $1,100 in health care per person for the nearly eight million Mexicans in the United States who are uninsured or on Medicaid, compared with the $535 per-person in health spending that Mexico devotes to each of its citizens still in Mexico. Although President Calderón has inveighed against the corporatist practices of the once-dominant PRI, he has embraced the leader of the corrupt National Union of Social Security Workers, whom the PAN has awarded a seat in the Chamber of Deputies. Nurtured under the PRI, the SNTSS bears a heavy responsibility for the skyrocketing costs of health care in a country that devotes only 6.1 percent of its GDP to this vital sector.
End Notes
1 Ronald Mortensen, “Obama Links Health Insurance Reform and Comprehensive Immigration Reform (Amnesty),” Center for Immigration Studies, September 20, 2009, http://cis.org/mortensen/insurance.
2 National Population Council of the Government of Mexico (CONAPO) et al., “Migration & Health: The Children of Mexican Immigrants in the United States,” October 2009, http://www.healthpolicy.ucla.edu/pubs/files/Ingles.pdf. Press release and other information at http://healthpolicy.ucla.edu/pubs/Publication.aspx?pubID=381.
3 “1.5 Million Immigrant Children Lack Health Insurance,” FNS (Frontera NorteSur) News, Center for Latin American and Border Studies New Mexico State University, Las Cruces, N.M., October 8, 2009.
4 The Calderón administration is in the process of liquidating the extraordinarily corrupt and inefficient LyFC, which serves Mexico City and areas of nearby states.
5 The March 2008 Current Population Survey (CPS) shows 11.62 million Mexican immigrants (legal and illegal) living in the United States, 6.33 million of whom are without health insurance. The CPS also shows 1.37 million Mexican immigrants on Medicaid, the U.S.-taxpayer-provided health insurance program for the poor. Based on earlier research, it is estimated that uninsured immigrants from Mexico receive about $613 per person a year in taxpayer-provided health care, primarily in emergency rooms and free clinics. This estimate takes into account the younger age and generally lower use of health care by immigrants. (See “Illegal Immigrants and HR 3200: Estimate of Potential Costs to Taxpayers,” www.cis.org/IllegalsAndHealthCareHR3200.) The CPS shows that the average Mexican immigrant on Medicaid costs taxpayers $3,600 a year. This means that the 66 percent (1.37 + 6.33 = 7.7 million) of Mexican immigrants who are on Medicaid or are uninsured receive on average $1,146 from American taxpayers for health care. My thanks to Steven Camarota, Director of Research, of the Center for Immigration Studies for this analysis.
6 “CNDH denucia problemas graves en sistema de salud,” El Universal, May 11, 2009.
7 Margarita Vega, “Critica OCDE dispersión en sistema de salud en México,” El Diario, August 1, 2009.
8 “IMSS pide usar reservas ante crisis económica,” Informador.com.mx, September 7, 2009.
9 Sergio Roterman Heldman, “Cartas del Lector/Olvido de IMSS,” Reforma, September 4, 2009.
10 This section benefits from Dudley Althaus, “Retirees Look South for Healthy Golden Years,” Houston Chronicle, December 9, 2007.
11 Quoted in Sheila Whyte, “How Mexico’s Health System Works,” CBC News, May 4, 2009.
12 John Rice, “Flu Exposes Flaws in Mexico’s Health Care System,” Associated Press, May 9, 2009.
13 Eduardo Portas, “Pega a IMSS infraestructura,” Reforma, August 8, 2007.
14 “Union Democracy?” Mexican Labor News and Analysis, March 2, 1998, www.ueinternational.org/vol3no5.html.
15 Quoted in Alvaro Delgado, “La nueva ficha del PAN, Valdemar Gutiérrez, vinculado al narco,” Proceso, April 14, 2009.
16 Daniel Pensamiento, “Toma líder protesta en sólo 25 segundos,” Reforma, October 27, 2006.
17 “(Desde Campeche) Denuncian actors de corrupción ante el líder nacional del SNTSS, Valdemar Gutiérrez Fragoso,” El Observador Campechano, December 4, 2008.
18 Ricardo Brussolo, “Empleados del IMSS demandan al sindicato por nepotismo,” Grupo Verbo Libre Editores, August 21, 2009, www.horacero.com.mx/noticia/index.asp?id=NHCVL18803.
19 “Tráfico de corneas en el IMSS,” Proceso, February 5, 2006.
20 Laura Carrillo, “Crece 30% costo de pensiones del IMSS,” El Diario, July 6, 2009.
21 Daniel Pensamiento, “Acapara sindicato nómina del IMSS,” Reforma, October 12, 2006.
22 Carrillo, “Crece 30% costo de pensiones del IMSS.”
23 See George W. Grayson, “‘Jimmy Hoffa in a Dress:’ Union Boss’s Stranglehold on Mexican Education Creates Immigration Fallout,” Center for Immigration Studies, April 2008, http://www.cis.org/mexican_education_fraud.html.
24 The PRI offered the SNTSS boss a third spot on its proportional representation list; the PAN gave him a second spot, which absolutely guaranteed his election.
25 Germán Martínez quoted in “Lo desecha el PRD, lo candidatea el PRI, se queda en el PAN,” Proceso, April 8, 2009.
26 “Decadence of the Elite,” Harvard International Review, May 18, 2009.
27 Ruth Rodríguez and Thelma Gómez Durán, “Sistema de salud, por los suelos,” El Universal, May 14, 2009.
28 Rice, “Flu Exposes Flaws in Mexico’s Health Care
System.”
29 “‘Negligencia criminal’ del IMSS y gobiernos en el caso ABC, dictamina la CNDH,” Proceso, July 30, 2009.