Panel: Healthcare for Illegal Immigrants: What would it cost?
Download a PDF of this Backgrounder.
Jason Richwine, PhD, is a public policy analyst based in Washington, D.C., and a contributing writer at National Review.
Summary
As presidential candidates debate whether illegal immigrants should receive government health benefits, it is important to understand how immigrants (both legal and illegal) currently benefit from Medicaid, the public healthcare program for the poor.
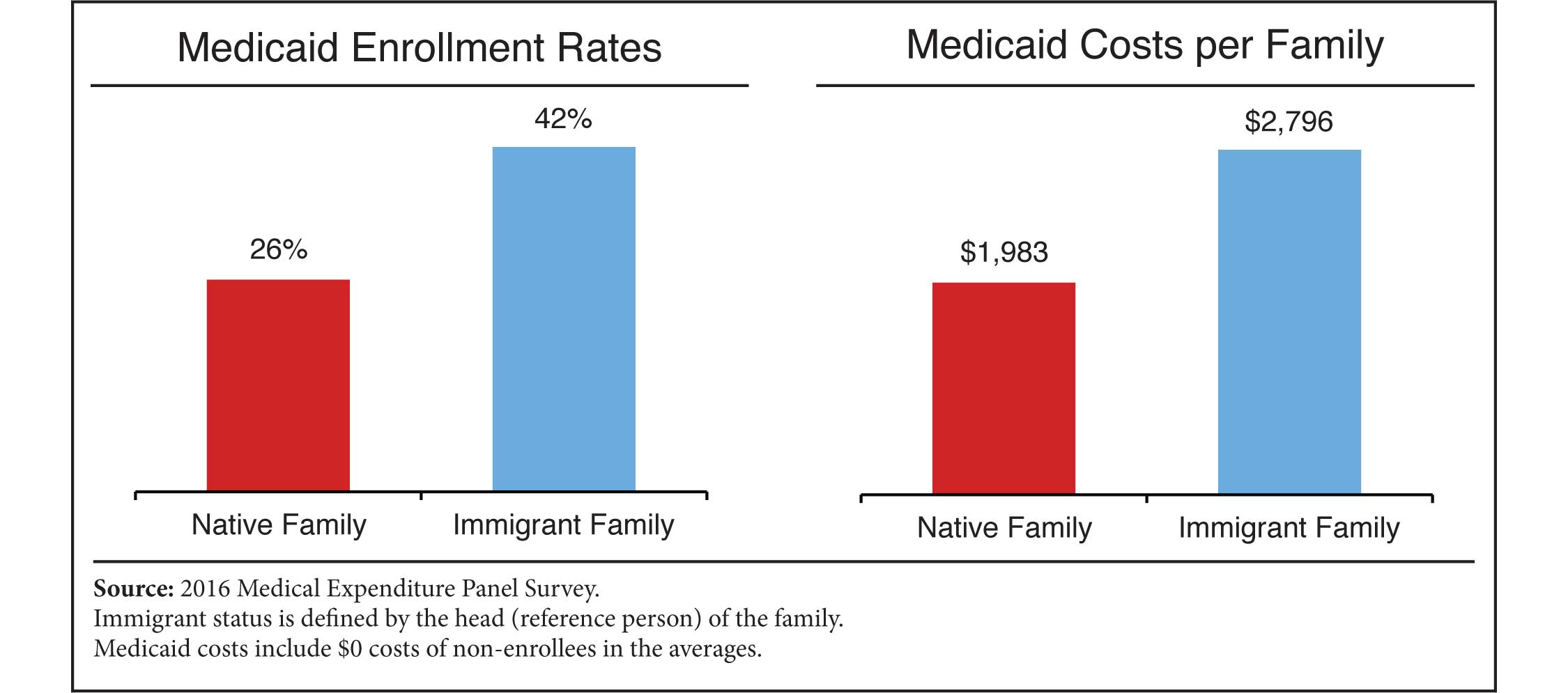
Using data from the Medical Expenditure Panel Survey, this report finds that 42 percent of immigrant-headed families had at least one member who was enrolled in Medicaid during 2016, compared to 26 percent of native-headed families. The average immigrant family created $2,796 in Medicaid costs, compared to $1,983 for the average native family.
Immigrants are costlier not because they have any special appetite for welfare, but because they tend to have less education and larger families that they struggle to support. All U.S. residents with those characteristics, foreign-born or native-born, are more likely to rely on government programs such as Medicaid. Immigrant welfare use can be reduced by changing selection criteria to favor immigrants who will have sufficient earning power to support their families without taxpayer assistance.
 |
Introduction
During their presidential debate on June 27, all 10 Democratic candidates on the stage raised their hands to affirm that they would open government healthcare benefits to illegal immigrants. When asked for specifics afterward, the candidates offered a range of proposals — from simply granting illegal immigrants unsubsidized access to the federal exchange, to giving them full public benefits under a "Medicare for All" system.1
In response to these proposals, the Center for Immigration Studies has issued two new reports. This first report details the participation rate and cost of Medicaid usage by immigrants under existing policy, which offers noncitizens less access to the program compared to citizens. A second report estimates the added cost of providing illegal immigrants full access to public health benefits, with most of the increase driven by exchange subsidies.2
Under existing policy, immigrant access to Medicaid is limited. Illegal immigrants, temporary immigrants (such as people on student or work visas), and immigrants who have been permanent residents for less than five years are generally not eligible. There are important exceptions to these rules, however. In many states, children and pregnant women can receive Medicaid without the five-year waiting period.3 Refugees and asylees are also eligible for Medicaid (or a similar program) without a waiting period, and all immigrants can receive emergency services regardless of status.
A final qualifier, and perhaps the most important one, is that U.S.-born minor children of immigrants are fully eligible for all public benefits, including Medicaid. As demonstrated in the results section below, immigrants and natives have similar rates of Medicaid use when considered as individuals, but immigrant families (which can include U.S.-born children) are significantly more likely than native families to have at least one member enrolled in Medicaid.
Data and Methods
Several datasets are available to compare the Medicaid use of immigrants and natives. The most well known is probably the Current Population Survey's Annual Social and Economic Supplement (ASEC), which asks respondents whether they used Medicaid during the prior calendar year. The ASEC undercounts program participation, however, in part because it asks respondents to recall their participation over a period between three and 15 months before the interview takes place. In addition, the ASEC measures only participation in Medicaid, not the cost of medical care charged to the program on behalf of each respondent.4
Alternatively, the Survey of Income and Program Participation (SIPP) follows respondents over time, asking them about their monthly program participation at different points throughout the year. The result is a more complete picture of welfare participation compared to what the ASEC provides. However, like the ASEC, the SIPP does not measure the cost of Medicaid — only participation in the program.5
This report employs a third option, the Medical Expenditure Panel Survey (MEPS). Like the SIPP, the MEPS follows respondents over time to achieve a comparably accurate estimate of Medicaid participation. Unlike the SIPP, however, the MEPS supplements its interviews with information from medical providers on the costs generated by respondents throughout the year. These costs are categorized (such as a doctor visit or a prescription medicine) and assigned a payer (such as Medicaid or private insurance). This report focuses on Medicaid, which is the largest public health program for the poor.6
The MEPS is clearly the best dataset for comparing Medicaid costs between immigrants and natives. (The MEPS records place of birth, so that "immigrants" includes all those born abroad, regardless of citizenship.) An important caveat, however, is that Medicaid expenditures reported in the MEPS do not account for all of the program's costs. Because the MEPS is based on health events experienced by individuals in the survey, general Medicaid funds — such as administrative costs, disproportionate share hospital payments, and other grants — are not counted. Furthermore, the MEPS samples only from the civilian non-institutionalized population, meaning the costs generated by Medicaid enrollees in nursing homes and hospice care are omitted. Finally, no survey is perfect, and the MEPS does suffer from some underreporting of Medicaid costs that it was designed to capture, particularly costs associated with transients and the homeless.7
The fact that the MEPS covers only the non-institutionalized population and omits administrative costs is inherent to the study design and cannot be altered. However, it is possible to adjust the MEPS data to include the costs that the survey was designed to capture but missed. In a study that reconciles the 2012 MEPS with administrative data on health spending, researchers from the Department of Health and Human Services (HHS) found that overall Medicaid spending reported in the 2012 MEPS was 35 percent lower than it should have been given the MEPS target population and the types of medical events it covers. The undercounts ranged from 16 percent to 82 percent among the seven subcategories of Medicaid spending, such as doctor visits and hospitalization.8 This report uses the HHS undercount figures to adjust MEPS costs upward to match administrative records.
In the sections that follow, Medicaid usage rates and costs are presented at both the individual level and the family level, with immigrant and native families distinguished by the nativity of the head (or "reference person") of the family. An immigrant family can have some U.S.-born members — including, most critically, U.S.-born children of immigrants. A family-level analysis allows for Medicaid use by U.S.-born minor children of immigrants to be properly counted in the immigrant column, not the native column. Although this accounting is sometimes disputed by immigration advocates, the case for it is clear. Because adults have a legal obligation to provide medical care to their minor children (and to any other dependents), Medicaid spending on children is effectively a financial transfer to their parents. Furthermore, Medicaid eligibility is generally determined by family income and family size.9 Individual-level results are provided in the next section for reference, but the family is the most relevant unit of comparison.
Main Results
Table 1 shows the percentage of Americans enrolled in Medicaid by immigration status, with the immigrant category further divided into subgroups. Despite restrictions on access, immigrant individuals use Medicaid at the same 23 percent rate as native individuals.10
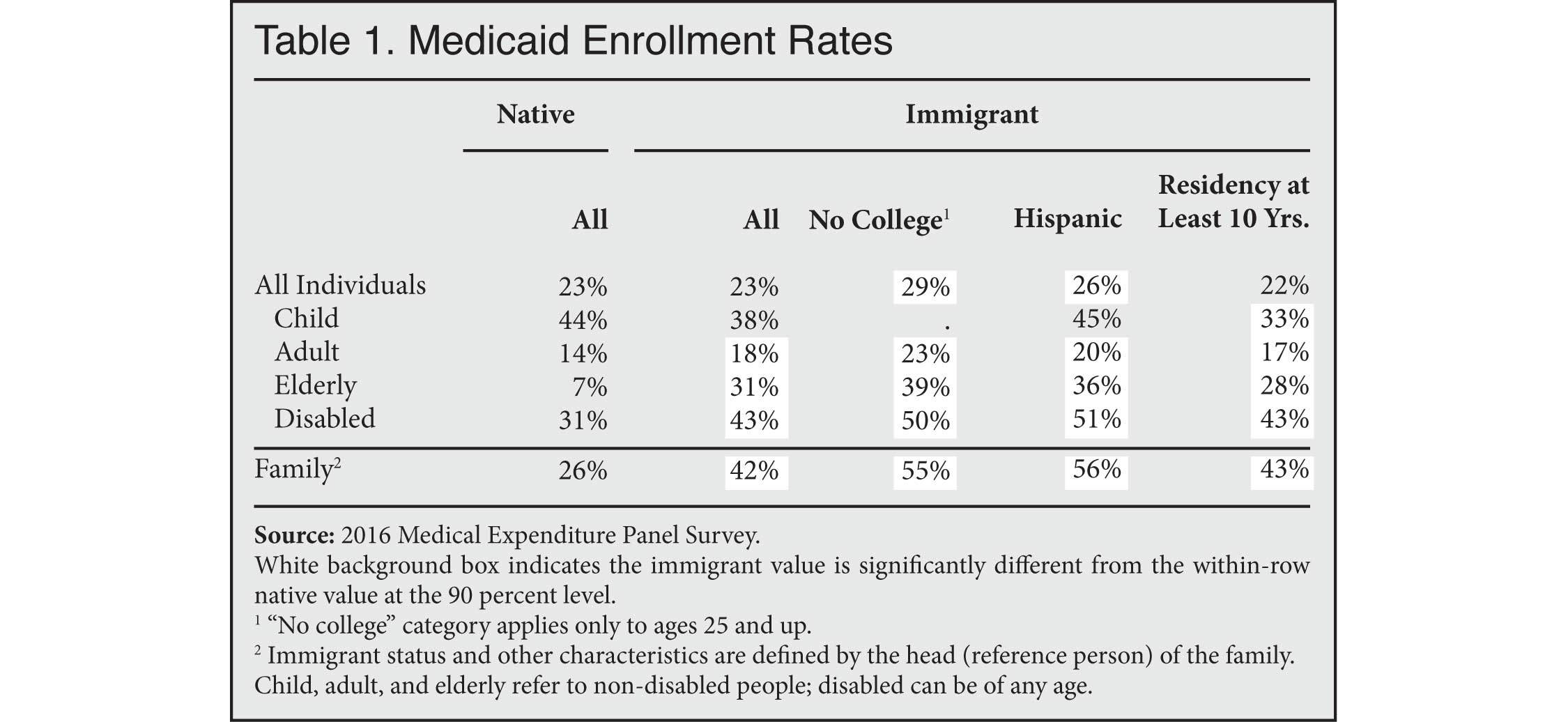 |
Immigrant children (of whom there are relatively few) appear less likely to use Medicaid than native children, but the difference is not statistically significant.11 Immigrant adults are significantly more likely to enroll than native adults. An especially large and significant disparity exists among the elderly, probably because some immigrants are not eligible for Medicare. In general, immigrants from Latin America and immigrants without a college degree have above average rates of Medicaid enrollment, while enrollment rates for immigrants with a residency of at least 10 years do not substantially differ from rates among immigrants overall.
As discussed earlier, the most informative comparison is at the family level. The last row of Table 1 indicates that 42 percent of immigrant families had at least one member enrolled in Medicaid, compared to 26 percent of native families.
How do these enrollment rates translate to costs? Table 2 shows how much the average immigrant individual or family costs in Medicaid expenditures compared to natives. These costs are averaged across all individuals or families regardless of whether they were enrolled in Medicaid. (In other words, many $0 values are included in the averages.) In addition, the costs are adjusted upward to account for underreporting in the MEPS, as discussed in the "Data and Methods" section.
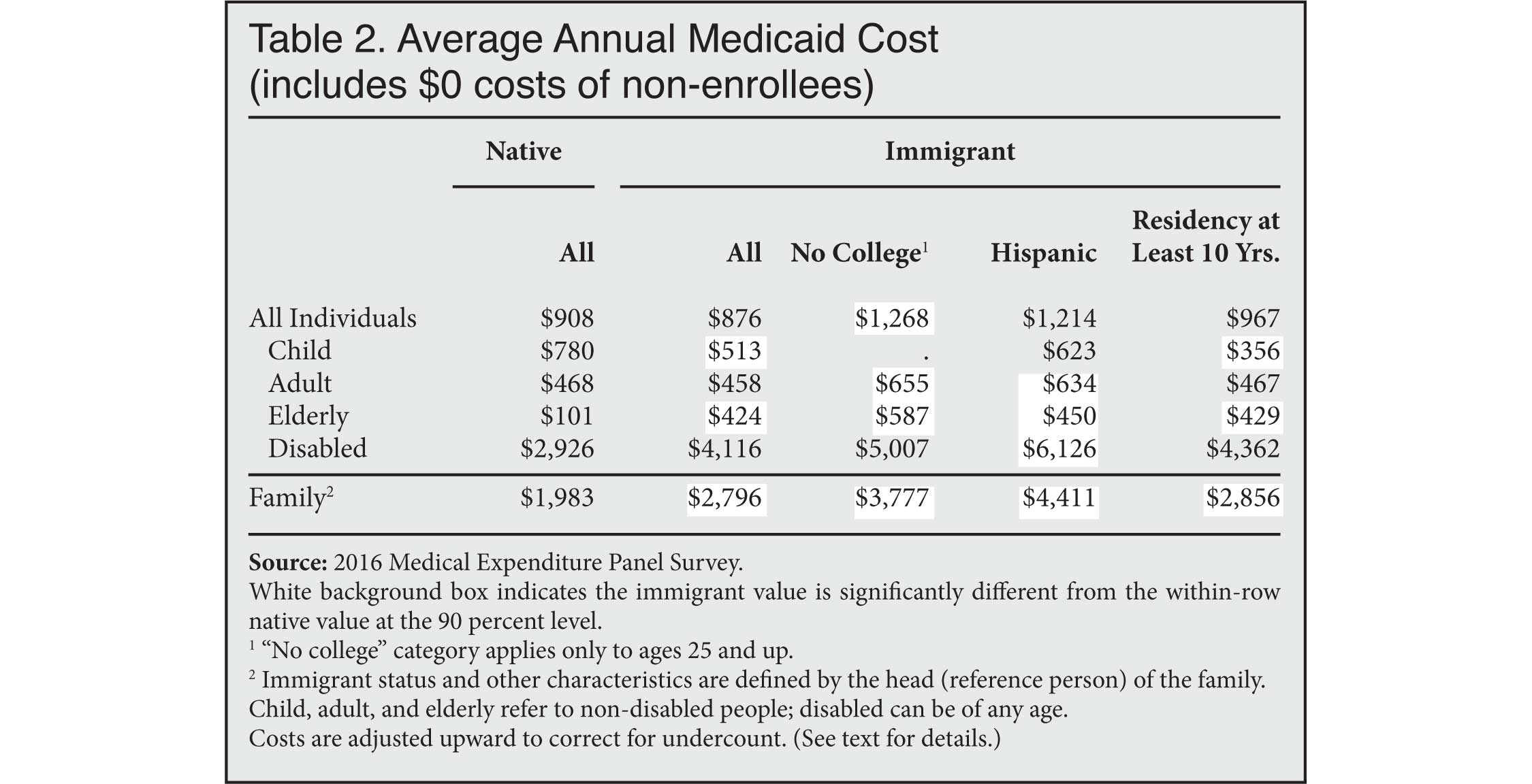 |
Native individuals cost insignificantly more than immigrant individuals on a per-capita basis. Among families, however, immigrants are significantly costlier, with an average Medicaid charge of $2,796 compared to $1,983 for native families. The costliest subgroup is Hispanic immigrant families at $4,411.
Why Are Immigrant Families Costlier?
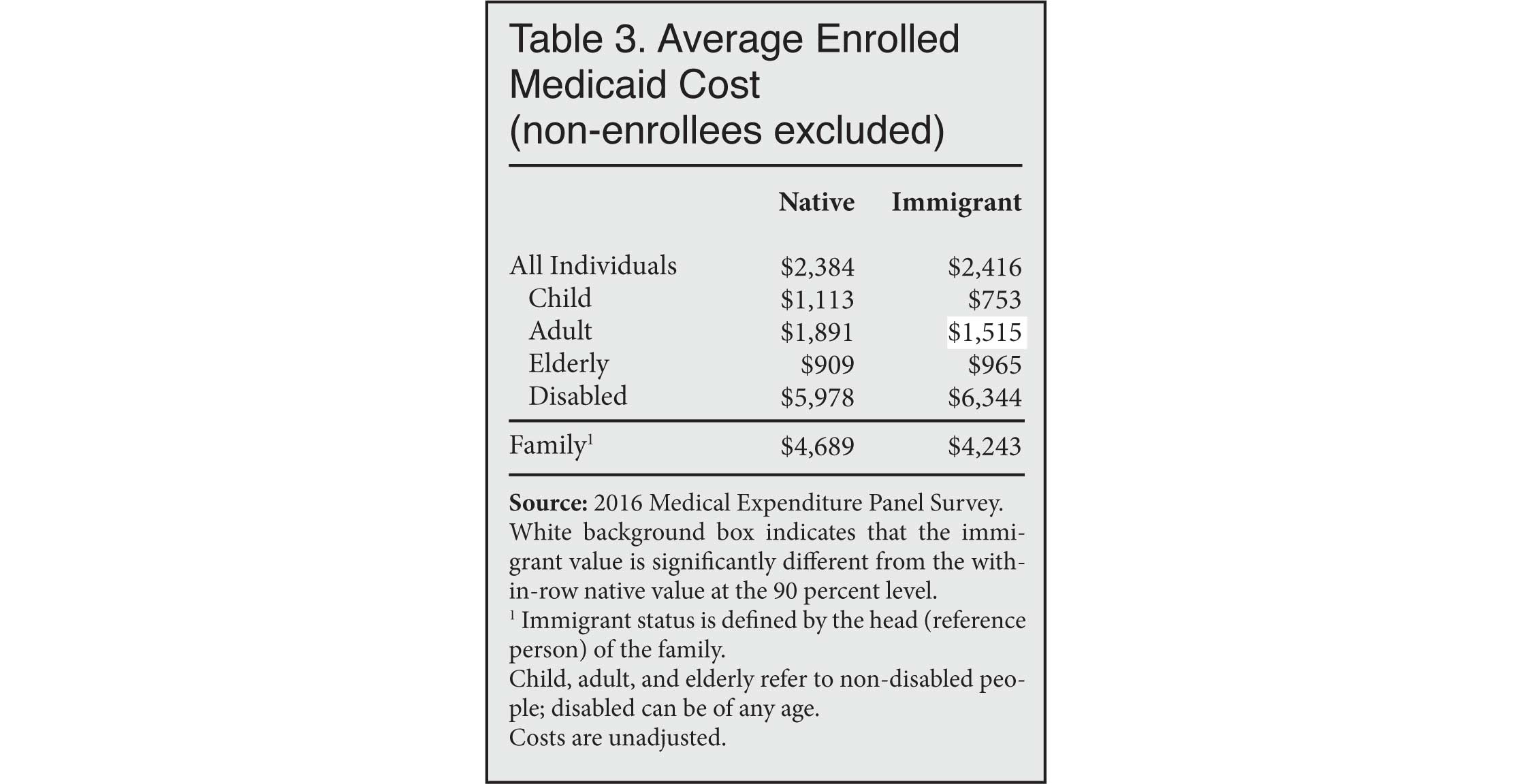
Do immigrant families consume more Medicaid dollars solely because of their higher enrollment rate, or do they also cost more once enrolled? Table 3 shows that among families that are enrolled, immigrant families are no more costly than native families.12 If anything, enrolled immigrant families cost less than enrolled native families, although the difference is not statistically significant.
 |
It is clear that the higher enrollment rate among immigrant families drives their higher overall Medicaid costs, but why do immigrant families enroll so much in the first place? Immigrants do not appear to have a special appetite for welfare compared to natives; rather, they are simply more likely to have the demographic profile associated with native use of Medicaid — namely, less education combined with larger families that they struggle to support. Table 4 uses regression analysis to show how the difference between immigrant and native Medicaid costs shrinks when these characteristics are taken into account.
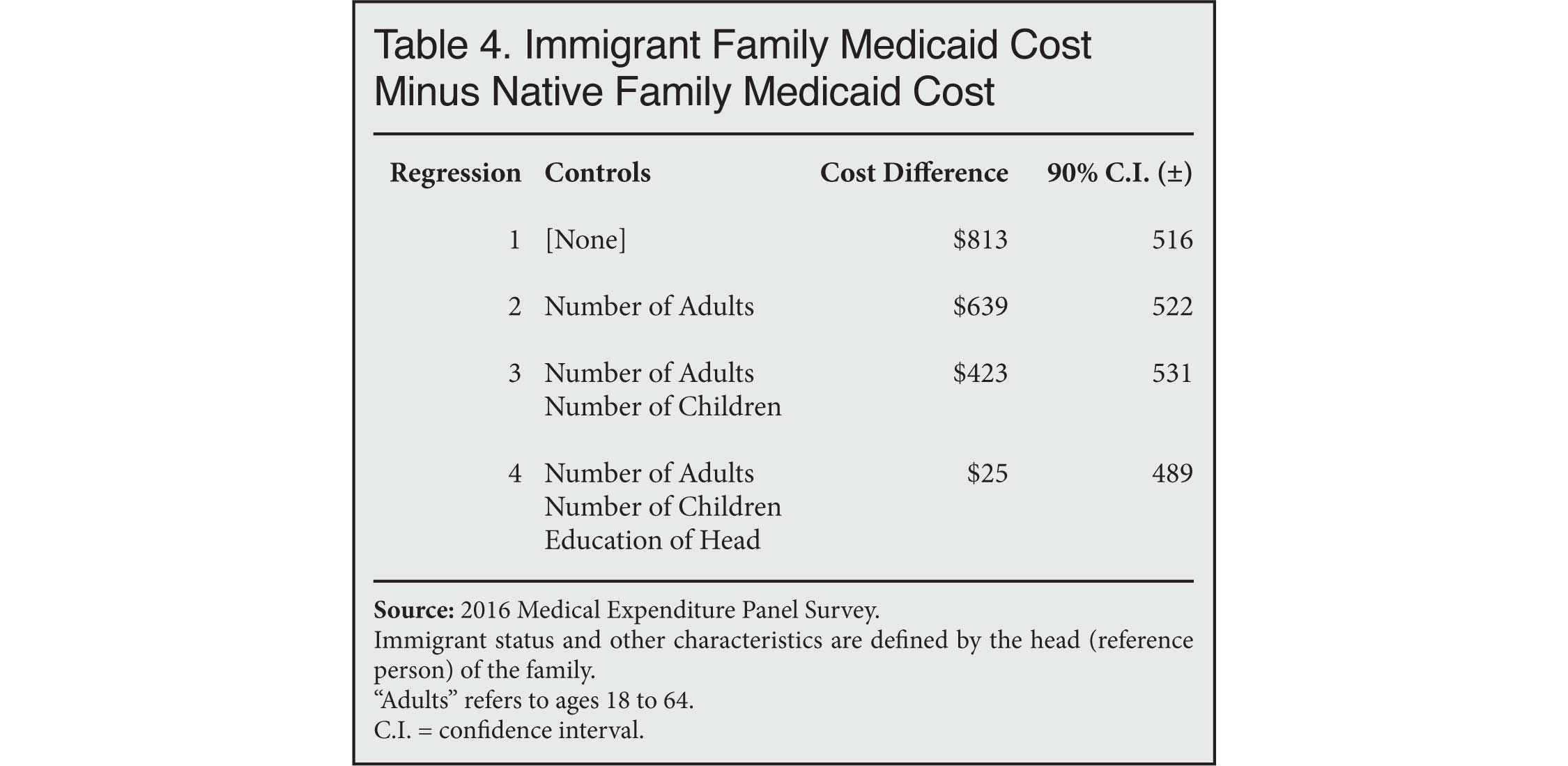 |
In the baseline estimate shown in the first row, immigrant families consume $813 more in Medicaid than native families, which is consistent with Table 2 above. The second row shows that the immigrant-native difference shrinks to $639 when controlling for the number of non-elderly adults in the family. The difference falls to $423 after adding a control for children in the third row. Finally, the fourth row shows that the difference becomes tiny and statistically insignificant when the education level of the family head (or reference person) is taken into account.
These results suggest that the problem of immigrants' reliance on Medicaid is not due to their foreign-born status per se; rather, it is the result of an insufficiently selective immigration policy that adds more people to the U.S. population who are less-educated and have larger families to provide for. As a result, a disproportionate share of immigrant families turn to the American taxpayer for support in the form of welfare programs, including Medicaid.13
Conclusion
As presidential candidates debate whether and to what extent illegal immigrants should receive government health benefits, the public should be aware of the Medicaid dollars that immigrants (legal and illegal) already consume, both for themselves and for their U.S.-born dependents. This report has shown that 42 percent of immigrant families had at least one member enrolled in Medicaid in 2016, compared to 26 percent of native families. The Medicaid cost per immigrant family (including non-enrollees) was $2,796, compared to $1,983 per native family.
The greater cost imposed by immigrants is entirely predicted by their relatively low levels of education and relatively large families. Whether they were born in Ohio or Guatemala, U.S. residents with those characteristics are at greater risk of relying on taxpayers to provide medical care to themselves, their dependents, or both. When immigration policy adds to the number of Americans who struggle to support their families, it adds to the welfare rolls as well.
Appendix
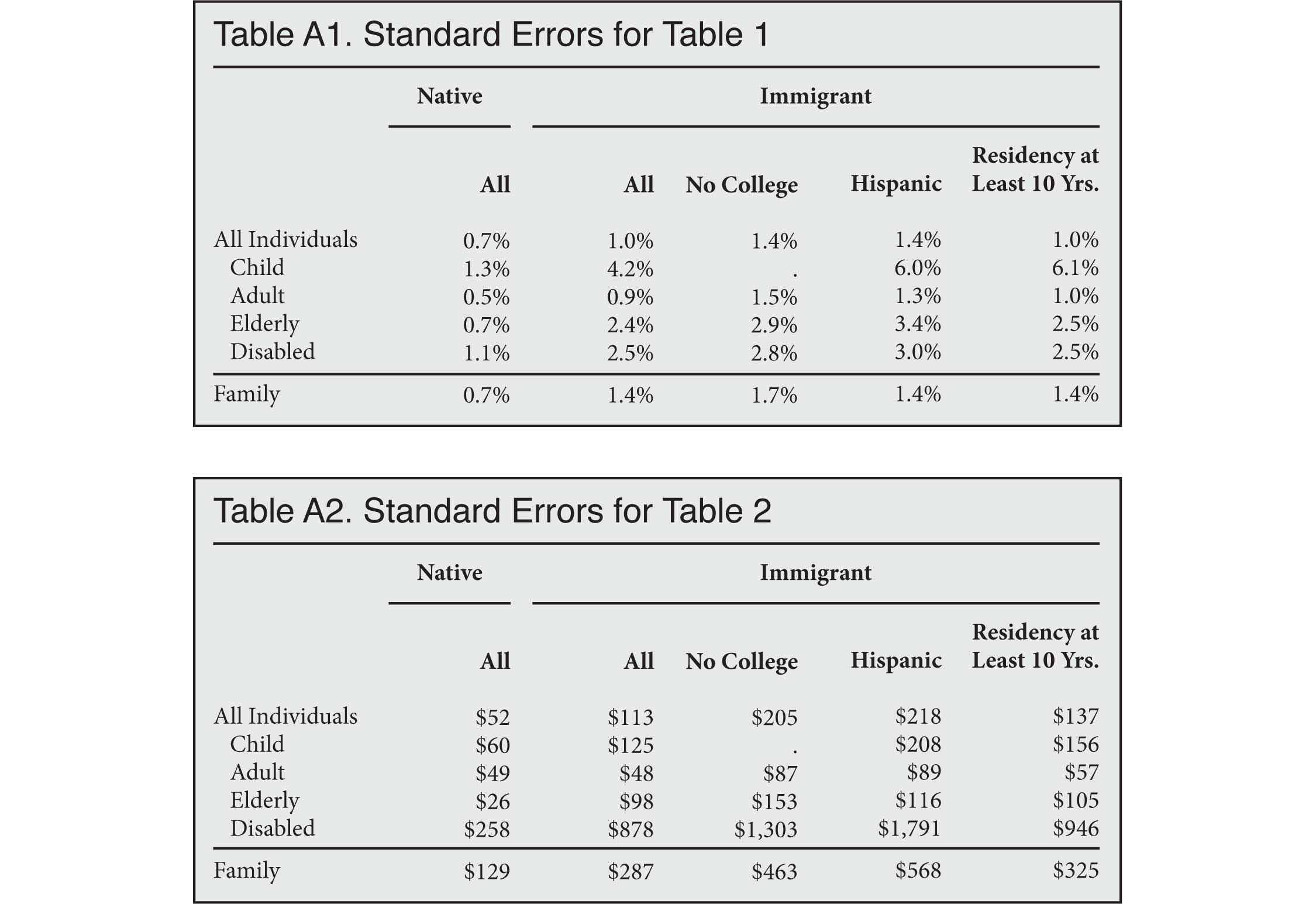
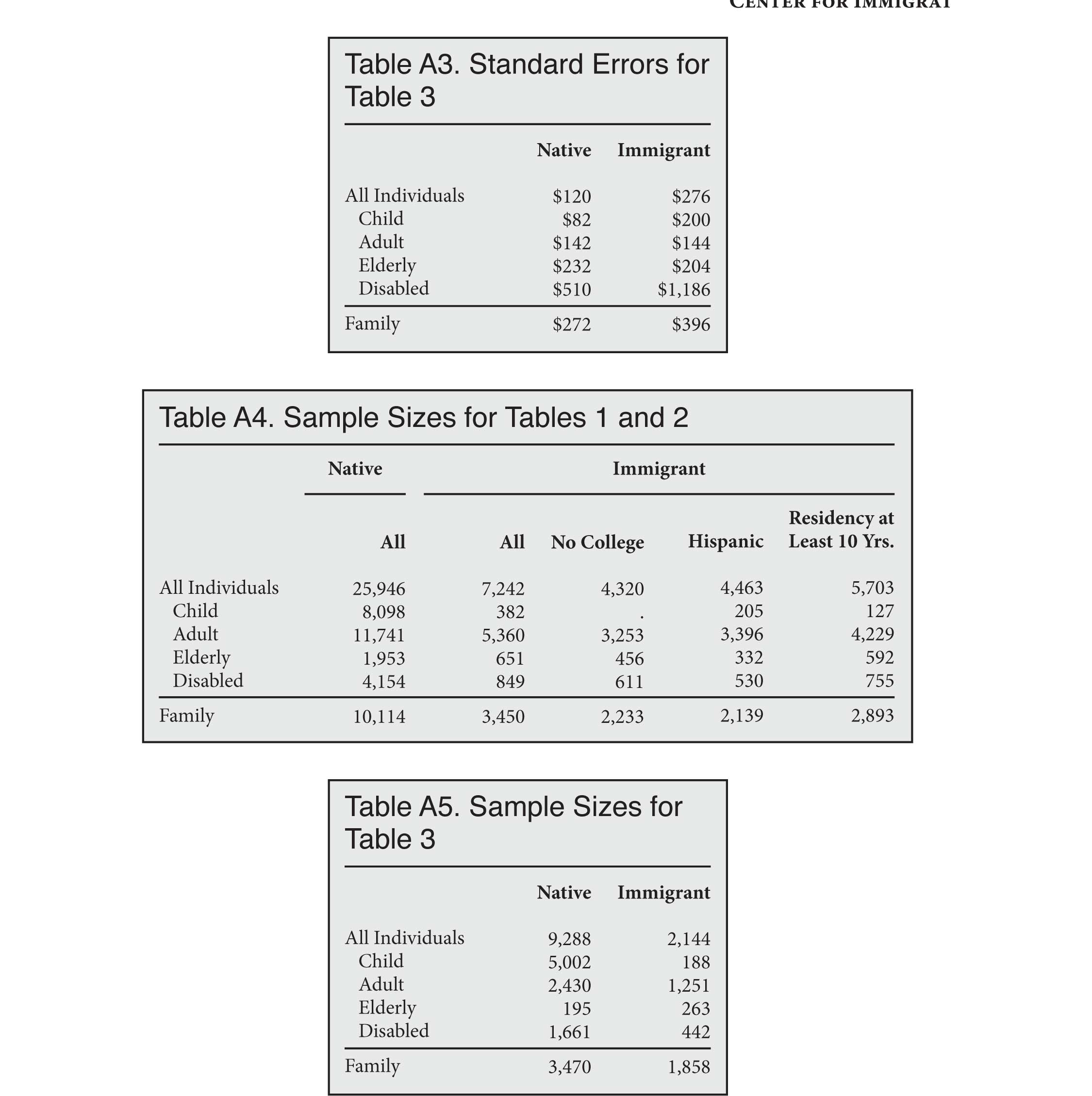
All standard errors are calculated using the complex survey weights that accompany the MEPS dataset.
 |
 |
End Notes
1 Ronald Brownstein, "The Democrats' Gamble on Health Care for the Undocumented", The Atlantic, July 11, 2019.
2 Steven Camarota, Karen Zeigler, and Jason Richwine, "How Much Would It Cost to Provide Health Insurance to Illegal Immigrants?", Center for Immigration Studies Backgrounder, October 2019.
3 As of the beginning of 2019, 25 states waive the five-year residency requirement for pregnant women who wish to enroll in Medicaid, and 34 states waive the residency requirement for immigrant children. See "Medicaid/CHIP Coverage of Lawfully-Residing Immigrant Children and Pregnant Women", Kaiser Family Foundation, January 1, 2019.
4 Before 2015, the ASEC included the "person market value" of Medicaid. However, this value was not an actual Medicaid cost for each respondent; rather, it was an average cost based on the respondent's age and disability status.
5 For an analysis that imputes Medicaid costs based on participation rates from the SIPP, see Jason Richwine, "The Cost of Welfare Use by Immigrant and Native Households", Center for Immigration Studies Backgrounder, May 9, 2016.
6 The Children's Health Insurance Program (CHIP) is an extension of traditional Medicaid and is included with Medicaid in the MEPS. This report also adds the MEPS category "Other Public" to Medicaid, as it represents "Medicaid payments reported for persons who were not reported to be enrolled in the Medicaid program at any time during the year." See: "MEPS HC-192 2016 Full Year Consolidated Data File," Agency for Healthcare Research and Quality", p. C-112.
7 In addition, fraudulent claims cost Medicaid billions of dollars every year, and these costs are not likely to be captured in the MEPS. See Didem M. Bernard, Cathy Cowan, Thomas M. Selden, David Lassman, and Aaron Catlin, "Reconciling Medical Expenditure Estimates from the MEPS and the NHEA, 2012", presented June 12, 2018, pp. 17-18.
8 Bernard et al., Table 6. The authors note that undercounts can change from year to year. Therefore, these undercount adjustments from 2012 should be considered merely estimates when applied to 2016 data. In fact, 2017 MEPS data became available before this report was finished, but changes in survey methods starting that year made the data too dissimilar to apply an older undercount adjustment.
9 In states that expanded Medicaid under the Affordable Care Act, anyone living at less than 138 percent of the poverty line is eligible. Poverty, of course, is determined by family income and family size. In states that have not expanded Medicaid, eligibility rules are more varied but still usually rely on a family-based poverty calculation.
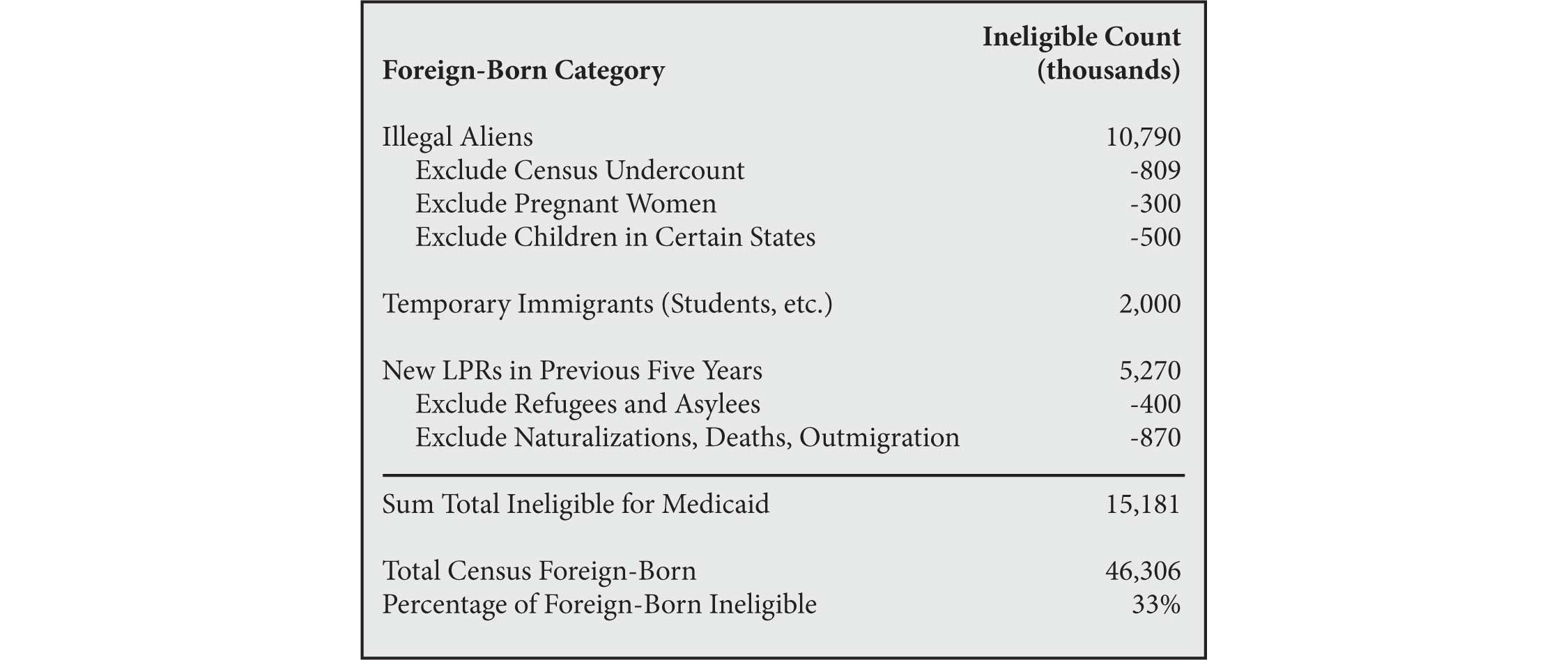
10 Since so many immigrants are not legally eligible for Medicaid even if they are poor, we can infer that a larger percentage of eligible immigrants use Medicaid compared to natives, all of whom are eligible if they meet the poverty criteria. A back-of-the-envelope calculation shown in the table below suggests that one third of immigrants are legally barred from using Medicaid (except for emergency services).
 |
To estimate the percentage of eligible immigrants who used non-emergency Medicaid in 2016, we want to exclude MEPS respondents who used only emergency services. Unfortunately, there is some ambiguity as to whether the MEPS will count an illegal alien who uses emergency services as "enrolled" in Medicaid. As discussed in Note 6, the MEPS includes an "Other Public" expenditure variable defined as "Medicaid payments reported for persons who were not reported to be enrolled in the Medicaid program at any time during the year", and respondents who have such a payment are counted as Medicaid users for purposes of Table 1. If we disregard respondents who have only "Other Public" expenditures and focus only on those whom the MEPS counts as officially enrolled in Medicaid, then Medicaid usage rates for immigrants and natives drop to 22 percent and 21 percent, respectively.
The rough estimate that one third of immigrants are legally ineligible for non-emergency Medicaid implies that the 22 percent of immigrants receiving non-emergency Medicaid are drawn from an eligible pool of two thirds of all immigrants. Therefore, 22/67 = 32.8 percent of eligible immigrants used Medicaid in 2016, compared to 21 percent of natives (who are all eligible).
11 The vast majority of immigrants arrive in the United States as adults. In the 2016 MEPS, just 5 percent of the foreign-born are under the age of 18, compared to 26 percent of the native-born.
12 Unlike the costs in Table 2, the costs in Table 3 are exactly as reported in the MEPS and are not adjusted upward for undercount. The reason is that part of the MEPS undercount is due to missing Medicaid enrollees entirely. Applying an upward adjustment to only the enrollees identified in the MEPS would overstate their costs.
13 The longstanding (but heretofore rarely enforced) law against admitting or granting permanent residency to an alien who is likely to become a "public charge" was recently strengthened. Participation in Medicaid is now considered evidence that someone is a public charge. However, the rule applies only to immigrants as individuals, not to their dependents. For example, the Associated Press recently profiled a low-income Mexican immigrant who has lived in the United States for more than two decades. He is not personally covered by Medicaid, but he has enrolled his two citizen children in the program. Even though he cannot afford medical care for his own children and has turned to the U.S. taxpayer for help, he is still not considered a "public charge" under the new rule. See Sophia Tareen, "Doctors Say New Rule Will Mean Sicker Immigrants", Associated Press, August 18, 2019; Jason Richwine, "Legitimizing the Public Charge Determination", December 6, 2018.