Table of Contents
Executive Summary
One of the most troubling social trends in recent years has been the rapid increase in the number of people without health insurance. According to the Census Bureau, since 1990 the uninsured population has grown by nearly 10 million and stood at 44.3 million—or one-sixth of the total U.S. population in 1998. Both presidential candidates have proposed major new initiatives costing billions of dollars per year to address the problem.
Efforts to explain the problem have generally focused on trends in employment practices, the rising costs of health care insurance, changes in eligibility for government programs, or the demographic characteristics of the uninsured. To date, relatively little effort has been focused on the impact of immigration policy on this problem. This paper examines the composition of persons without health insurance using the latest data available from the Census Bureau. The findings indicate that while other factors have contributed to the problem, immigration has had an enormous impact on the size and growth of the uninsured population in the United States.
Findings
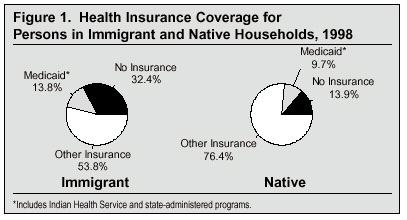
- In 1998, 32.4 percent of persons living in immigrant households (primarily immigrants and their children) lacked health insurance—more than twice the 13.9 percent of persons in native households without insurance.
- Immigrants who arrived between 1994 and 1998 and their children accounted for 59 percent (2.7 million people) of the growth in the size of the uninsured population since 1993.
- The impact of immigration on the overall size of the uninsured population is dramatic. The total uninsured population is one-third larger (32.7 million versus 44.3 million) when the 11.6 million persons in immigrant households without insurance are counted.
- Immigration has made it much more difficult to reduce the size of the uninsured population. For example, in just the last few years immigration has increased the number of uninsured children in the United States by 700,000, enough to offset most of the gains made so far under the State Children’s Health Insurance Program (SCHIP) enacted by Congress in 1997 at a cost of $4 billion a year.
- Although they comprise 13.1 percent of the nation’s total population, persons in immigrant households now account for 26.1 percent of the nation’s uninsured.
- Lack of insurance remains a severe problem even after immigrants have been in the country for many years. In 1998, 37 percent of immigrants who entered in the 1980s still had not acquired health insurance, and 27.2 percent of immigrants who entered in the 1970s remained uninsured.
- The lack of insurance coverage associated with immigrants is primarily explained by their much lower levels of education and their resulting higher poverty rates relative to natives. Because of the limited value of their labor in an economy that increasingly demands educated workers, many immigrants hold jobs that do not offer health insurance and their comparatively low incomes make it very difficult for them to purchase insurance on their own.
- Low levels of education and a high incidence of poverty do not account for all of the difference between immigrant and native households. Even educated and higher income immigrant households are much more likely to be uninsured than similarly situated natives.
- Continued high rates of Medicaid use (Figure 1) among immigrants coupled with low levels of insurance coverage means that almost half (46.2 percent) of persons in immigrant households either have no insurance or have it provided to them at taxpayer expense.
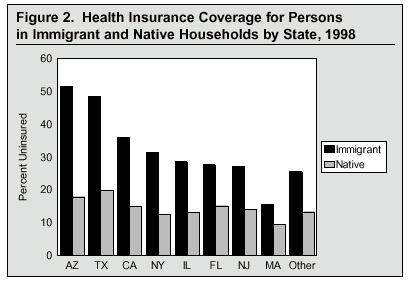
- In every major immigrant-receiving state and metropolitan area in the country, persons in immigrant households are dramatically more likely to be without health insurance than persons in native households (see Figure 2).
- Health insurance coverage varies significantly by country. Households headed by immigrants from Mexico, Central and South America, and Korea are the least likely to have health insurance, while those from Europe, Canada, and the Philippines are the most likely to be insured.
Factors Not Accounting for the Lack of Insurance Coverage Associated with Immigrants
- Although a very high percentage of illegal aliens do not have health insurance, they comprise only an estimated 26.8 percent of the uninsured living in immigrant households.
- The denial of benefits to some legal immigrants enacted as part of the1996 welfare reform legislation is not the reason so many persons in immigrants households do not have health insurance. Before welfare reform was enacted, nearly 31 percent of persons in immigrant households lacked health insurance, very similar to the current rate. Moreover, immigrant households continue to use Medicaid at higher rates than native households.
- The high percentage of persons in immigrant households without insurance is not explained by the presence of humanitarian immigrants (refugees and asylees). Because they have immediate access to the welfare system, including Medicaid, these immigrants and their children are somewhat more likely to have insurance than are other immigrants.
Why Study Immigration’s Impact on the Size of the Uninsured Population?
One may reasonably ask what effect, if any, does a larger national or local uninsured population have, especially for the majority of the population who do have health insurance? In addition to altruism, there are a number of very practical reasons to be concerned about the level of health insurance coverage in America and the role that immigration policy may be playing in this growing problem.
Impact on the Uninsured Already Here
The most obvious reason for concern is that by increasing the size of the uninsured population, immigration makes it much more difficult to help the uninsured already here. A recent study jointly released by the National Academy of Sciences and the Institute of Medicine concluded that the viability of care providers to the uninsured is more at risk today than ever before partly because of the growing size of the uninsured population. The cost of efforts to provide insurance or just basic care to the uninsured is dependent on the number of people in need of such assistance. If immigration increases the number of people who require government-financed health care, then the total cost of such efforts must grow accordingly. This can only reduce political support for such efforts. Alternately, if federal, state, and local outlays for the uninsured remain the same, then the level of services provided to each recipient must be reduced. This, too, is certainly not in the interest of America’s uninsured. Therefore, if one is concerned about the uninsured already here, significantly increasing the size of the uninsured population is certainly counterproductive.
Effect on Taxpayers
Although they do not have insurance, the uninsured still become sick or injured and require medical care. In many cases, the cost of providing medical services to the uninsured is paid by federal, state, and local governments. Many counties and cities that operate public hospitals and/or clinics and which provide services to the uninsured devote a sizable portion of their total budgets to the uninsured. In addition, health care providers are often reimbursed by the federal government for costs incurred treating the uninsured. While no definitive estimate exists for the reimbursement, it is likely that between $15 and $30 billion a year is spent on the uninsured by government at all levels. These costs do not include the more than $150 billion spent annually to provide Medicaid coverage to low-income residents.
Higher Premiums and Costs for Those with Insurance
While governments at all levels do compensate health care providers for some of the care given to the uninsured, a significant share is not compensated. Providers of health care to the uninsured simply cannot absorb all of the costs of providing such charity care, so they pass at least some of the costs along to paying customers in the form of higher prices for treatment, which in turn creates higher insurance premiums for those with insurance. Thus, a growing uninsured population creates a vicious cycle by driving up premiums, thereby reducing the number of employers who can afford to provide insurance. Additionally, higher premiums push the costs of insurance out of reach for many Americans who must purchase coverage on their own.
Increasing the Risk for the Spread of Communicable Diseases
Because they often do not receive routine preventive care and often seek out medical attention only when their condition is more serious, the uninsured unintentionally extend the period of time the public is exposed to communicable diseases. This problem is of particular concern among immigrants, because most come from developing countries where communicable diseases are more common.
Implications for Immigrant and Immigration Policy
Evaluating health insurance coverage among immigrants and their children is important because it is one way of assessing the consequences of immigration policy. It also affords us the best idea of how immigrants admitted in the future are likely to do if current immigration policy remains unchanged. Low rates of coverage imply that a significant proportion of immigrants have not successfully adapted to life in their new country, at least with regard to health insurance. This is important because without a change in immigration policy, the Census Bureau projects that 11 million new immigrants will likely settle permanently in the United States in just the next decade. If current trends continue, immigration may add an additional three to four million people to the ranks of the uninsured over the next 10 years.
In addition to immigration policy, which is concerned with who may come and how many, there is immigrant policy, which deals with how we treat the foreign-born, living in United States. Examining health insurance coverage among immigrants is important because if a large percentage of immigrants and their children already here lack insurance, we must deal with this problem in a constructive manner, whatever immigration policy is adopted in the future.
Methods and Data
Definitions and Data
The data for this study come from the March 1999 Current Population Survey (CPS) collected by the Census Bureau. The 1999 CPS offers the most recent data available and is the source of most official government statistics on the uninsured. Moreover, it is one of the best sources of information on persons born outside of the United States—referred to as foreign-born by the Census Bureau. For the purposes of this report, foreign-born and immigrant are used synonymously.
This report relies on the definition of insurance used in the government’s publication on health insurance, Health Insurance Coverage 1998: Current Population Report P60-208. Persons are considered to have health insurance if they were covered by insurance in the year prior to the survey provided by an employer, a family member’s policy, the government (primarily Medicaid and Medicare), or insurance they purchased themselves. Because the survey was conducted in March of 1999, it measures insurance coverage for 1998.
Methods
This study examines insurance coverage for persons living in immigrant- and native-headed households. Individuals related to the household head by blood, marriage, or adoption, regardless of their own nativity, are considered to be in an immigrant or native household based on whether the household head is foreign-born or native. Individuals who are unrelated to the head are considered immigrant or native based on the nativity of the head of the family in which they reside. For example, a foreign-born husband and wife (one would be the head) with two young U.S.-born children are counted as four people living in an immigrant household. If the same family rents a room to an unrelated native-born woman with a child of her own, then the women and her child would be counted as a separate native household. Individuals who live by themselves or who live with others to whom they are unrelated are in effect their own households and are considered immigrant or native based on their own nativity. Households are defined in this way so that they more accurately reflect the kind of income sharing and insurance eligibility that exists among members of the same family. Using this definition of household, 92.4 percent of the people living in immigrant-headed households were immigrants themselves or the U.S.-born child (under 21) of an immigrant parent. Therefore, this approach primarily measures insurance coverage for immigrants and their children. Because a child’s standard of living, including access to health insurance, is a function of his or her parents’ income, this method captures the full effect of immigration on the size of the uninsured population in the United States.
Policy Implications
The findings in this paper clearly show that immigration policy has significantly increased the size of the uninsured population in the United States. Assuming that policymakers are concerned about this situation, two sets of policy options would seem to merit consideration. The first set of options might involve a new immigration policy that reduces the flow of immigrants who are likely end up among the ranks of the uninsured. This would help to ensure that immigration does not continue to add to the health insurance problem in the future. The second set of policy options would involve the development and implementation of policies that address the needs of uninsured immigrants and their children already here.
Changing Immigration Policy
The lack of insurance coverage among immigrants stems primarily from their low levels of education and high poverty rates. Because of the limited value of their labor in an economy that increasingly demands a highly educated workforce, workers with few years of schooling are the most likely to hold jobs that pay poverty level wages and do not offer health insurance. Given their limited income, less-skilled workers are also often unable to afford coverage when it is not provided by an employer. In 1998, for example, 19 percent of college-educated adults in immigrant households were uninsured, compared to 53 percent of high school dropouts. Therefore, selecting more immigrants based on their skills would increase the percentage of new arrivals in the future who are able to obtain insurance.
Of course, there are benefits from immigration, and these might be enough to offset the costs associated with the dramatic increase in the uninsured population caused by immigration. In 1997, the National Research Council (NRC) examined the economic effects of immigration and concluded that by holding down the wages of the lowest-skilled workers, immigration creates a very small net benefit to the United States. Of course, lowering the wages of the poorest workers may be viewed by many as a cost rather than a benefit. Moreover, the NRC also found that the net drain on public coffers (tax payments minus services used) from immigrant households is enough to offset entirely the small positive economic effects. While opinions over the costs and benefits of immigration differ, the NRC report does make clear that we can curtail immigration without any worry that it will harm the U.S. economy.
Changing Legal Immigration. In most years, 65 to 70 percent of the 700,000 to 900,000 visas awarded are allotted to the family members of U.S. citizens and lawful permanent residents (LPRs). The Commission on Immigration Reform chaired by the late Barbara Jordan suggested limiting family immigration to the spouses, minor children, and parents of citizens and the spouses and minor children of LPRs—eliminating the preferences for the siblings and adult children of citizens and LPRs as well as the visa lottery. The preference for the spouses and children of non-citizens should also probably be eliminated, since these provisions apply to family members acquired after the alien has received a green card, but before he or she has become a citizen. If the parents of citizens were also eliminated as a category, family immigration would be lowered to roughly 200,000 to 300,000 per year. Humanitarian immigration should also undergo some changes. While the system must remain flexible, and in some years may need to expand well beyond the 50,000 originally intended by the Refugee Act of 1980, keeping refugee admissions at around this level would still allow the United States to take in nearly all of the persons identified by the U.N. High Commissioner for Refugees as needing permanent resettlement. The aforementioned changes would significantly reduce the number of legal immigrants admitted each year without regard to their ability to compete in the U.S. economy. Even with these changes, the United States would continue to accept more than twice as many immigrants as any other country.
Reducing Illegal Immigration. While the overwhelming majority of people living in immigrant households without insurance are legal immigrants or are the U.S.-born children of immigrants, reducing illegal immigration would still be helpful in lowering the number of immigrants entering each year who do not have health insurance. Illegal immigration is undoubtedly the lowest-skilled immigration, with an estimated two-thirds having no health insurance. There is broad agreement that cutting illegal immigrants off from jobs offers the best hope of reducing illegal immigration. Doing so requires three steps: First, a national computerized system needs to be implemented that allows employers to quickly verify that persons are legally entitled to work in the United States. Second, Congress needs to provide more funding so the Immigration and Nationalization Service (INS) can increase worksite enforcement efforts. Third, despite recent increases in funding, more could be done at the border. Controlling the border with Mexico would require perhaps 20,000 agents and the development of a system of formidable fences and other barriers.
The cuts in legal immigration proposed earlier would also help reduce illegal immigration because there are approximately four million people waiting their turn to receive the limited number of visas available each year in the various family categories. Such a system encourages people to simply come to the United States and settle illegally in anticipation of the day their visa is issued. Eliminating the sibling and adult children categories would do away with the huge waiting lists. In the long run, cutting legal immigration would also be very helpful in controlling illegal immigration because recent legal immigrants serve as magnets for illegal immigrants, providing housing, jobs, and entree to America.
Increasing Insurance Coverage Among Immigrants Already in the Country
While lowering the number of less-skilled legal and illegal immigrants entering each year would ensure that fewer immigrants admitted in the future end up among the ranks of the uninsured, it would not immediately increase the rate of insurance coverage among immigrants and their children currently residing in the United States. The most direct and simplest way to provide health insurance to persons in immigrant households would be for the government to provide it. Of course, the primary disadvantage of this approach is the cost. Health coverage for the more than 30 million recipients of Medicaid currently amounts to more than $150 billion a year. Providing coverage to the 11.6 million uninsured in immigrant households, or even only the 7.4 million who live in or near poverty, to say nothing of the poor in native households, would cost billions of dollars a year.
Even if providing coverage to all of the uninsured with low-incomes, including those in immigrant households, is thought to be prohibitively expensive, more can be done to increase their rate of insurance coverage. As we have seen, most persons without health insurance live in households where at least one person works. Thus, one set of options that could be pursued would involve changing regulations and tax policy with the intent of making it less expensive for businesses to provide insurance. In addition, both candidates for president have proposed tax credits for the working poor and near-poor so that they can more easily purchase private health insurance if it is not provided by an employer. So as to contain costs, efforts to provide insurance or tax credits could be specifically targeted at subgroups of the uninsured, such as children or those with the lowest incomes. The new State Children’s Health Insurance Program (SCHIP), enacted by Congress in 1997 at an annual cost of $4 billion, is one such effort. By April of 2000, SCHIP had insured an estimated one million of the 2.5 million low-income children who are eligible. As SCHIP shows, even providing insurance coverage to only a small fraction of the uninsured will not be cheap. It also highlights the necessity of changing immigration policy so that it does not continue to add to the problem.
Conclusion
In any discussion of the impact of immigration on the size of the uninsured population, it is important to keep in mind that immigration is different from other factors that have contributed to the problem because it is a discretionary policy of the federal government. The federal government controls both legal immigration and the level of funding to control illegal immigration. Even if it were desirable, Congress cannot legislate a pause in the advance of medical technology or easily reduce the strong demand for health care in an aging and increasingly secular society, both of which have driven up costs. But it can change immigration policy.
Why Has the Problem Been Ignored?
Part of the reason policymakers and researchers interested in health insurance coverage have not devoted much attention to immigration’s role in this growing problem is that they have generally been focused on other issues such as rising health care costs, changing employment practices, and Medicaid eligibility. In addition, only in 1994 did the Census Bureau begin to ask a nativity question on a regular basis as part of the CPS, making it possible to measure the impact of immigration. Moreover, immigrants are not politically powerful, so politicians can ignore them without paying much of a political price. Additionally, elected officials may be reluctant to call attention to the fact that a policy they have either supported or at least not tried to modify has led to an enormous growth in the uninsured population.
Another important reason the problem has not received the attention it should stems from the fact that most of the advocates for immigrants are also advocates for the current high level of immigration. These advocacy groups cannot call too much attention to the fact that immigration is responsible for a large share of the growth in the uninsured population because to do so would highlight a fundamental problem with the very policy they work so hard to keep in place. Calling for costly new programs to provide health coverage to immigrants would undermine the argument made by the advocates that high immigration is an economic and fiscal boon to the country. This conflict of interest between being an advocate for immigrants and an advocate for mass immigration means that relatively little attention is paid to the millions of immigrants and their children without adequate health care.
A Problem that Cannot be Ignored
While some may be tempted to ignore the lack of health insurance among immigrants and their children at a time of relative prosperity, this seems very unwise. In just the last four years immigration has increased the size of the uninsured population by 2.7 million people. Without a change in immigration policy and greater efforts to increase health care coverage among immigrant families already in the country, the problem will only grow much worse. The implications of this situation for the immigrants themselves, their children, the nation’s health care system, and society are too important to ignore.
Introduction
A large body of research indicates that, at least since 1987, both the number and percentage of U.S. residents who do have health insurance has been on the rise (Fronstin, 1998; Lewis, Ellwood, and Czajka, 1998). In 1999, the Census Bureau reported that nearly one out of six persons in the United States lacked health insurance in 1998, and the total size of the uninsured population now stands at more than 44 million (Campbell, 1999). Health care in general and the problem of the uninsured in particular have become the subject of intense national debate and the discussion over what to do about the uninsured has taken center stage in the current presidential race. Both presidential candidates have made major policy speeches on the subject and proposed significant new initiatives to deal to with the growing problem. Governor Bush has proposed tax credits costing an estimated $34.7 billion over five years to low-income families so that they can afford to purchase insurance. Vice President Gore has also proposed tax credits for the uninsured as well as an expansion of the Medicaid system, with an estimated total cost of $146 billion over 10 years (Mitchell, 2000). As these and other proposals suggest, fixing the problem is likely to be very costly, no matter what solutions are envisioned.
The increase in the size of the uninsured population has grown worse throughout the 1990s, despite a strong economy and the lowest unemployment rate in years. Examinations of the problem have generally focused on broad trends in employment practices, the costs of health care and health insurance, changes in eligibility for Medicaid and other government programs, or the socio-demographic characteristics of the uninsured (Fronstin, 1998; Budetti et al., 1999; Lewin and Altman, 2000; Holahan and Brennan, 2000). To date, however, relatively little effort has been made to evaluate the impact of immigration policy on the size of the uninsured population. This report looks at the composition of persons without health insurance. The findings indicate that nearly one in three persons living in households headed by immigrants (primarily immigrants and their children) have no health insurance and that immigrant households now account for one-fourth of the uninsured. Moreover, newly arrived immigrants and their children account for more than half of the growth in the size of the uninsured population in recent years. Immigration policy has become central to understanding the growing health care insurance problem in the United States.
Trends in Health Insurance
Prior to the Second World War, few Americans had health insurance of any kind. Because of wage controls imposed during the war, employers began to offer non-wage compensation, such as health insurance, in an effort to attract and retain workers (Styring and Jonas, 1999; Health Policy Consensus Group, 1999). Early on, the Internal Revenue Service ruled that such compensation was not taxable. This made and continues to make employer-provided health insurance more favored as a means of insurance purchase than for individuals to buy their own insurance with after-tax dollars. As a result, employers became the primary source for health insurance for most Americans in the workforce. From the 1940s on, health insurance primarily took the form of a fee-for-service coverage system under which health care providers were paid by insurance companies for each treatment given. The lack of cost controls in the fee-for-service system, demand for expensive new technologies and treatments, heavy government spending on health care, and other factors created upward pressure on health care cost in the 1980s that reached double-digit annual increases by 1990. Because of rising costs, many employers turned to managed care to insure employees.
While managed care has been partly successful in stemming the rise in health care costs, insurance remains very expensive. This has made it much more difficult for employers, especially small businesses, to provide coverage. As a result, fewer employers offer health insurance today than in the recent past. Moreover, many employers who do offer health insurance now pass along a larger share of the costs to employees. Because of the limited value of their labor in an economy that increasingly demands educated workers, less-skilled workers in particular are the most likely to hold jobs that do not have health insurance as a fringe benefit or, if insurance is offered, the employee must pay a large share of the costs. Those under the age of 65 whose employers do not provide health insurance, must purchase it for themselves and their children if they are not covered by another family member’s insurance or if they are not eligible for government-provided insurance under the Medicaid or SCHIP systems. Because individually purchased policies, in most cases, are bought with after-tax dollars and are not granted the same full tax deductibility and groups rates available to employers, individual plans can be prohibitively expensive. This, of course, is especially true for low-wage workers and their families, who are the least likely to be in a position to afford private insurance and who may choose not to accept insurance offered by their employers if a large percentage of the costs is borne by the worker (Campbell, 1999; Styring and Jonas, 1999; Health Policy Consensus Group, 1999).
Over the last decade the Census Bureau has tracked the size of the uninsured population using the Current Population Survey. In 1987 an estimated 31 million U.S. residents lacked insurance. Since 1987, the size of the uninsured population has grown by more than one million people per year on average. Moreover, the proportion of the population lacking health insurance has increased from 12.9 percent of the population in 1987 to 16.3 in 1998. This increase continued even after the recession of the early 1990s. Between 1992 and 1998, the size of the uninsured population grew by 5.6 million and the proportion of the population without insurance increased by 1.3 percentage points. This increase in the uninsured population has puzzled some health care experts because the generally favorable economic condition for most of the 1990s reduced unemployment and should have created pressure on employers to offer health insurance as a means of attracting and retaining workers in a tight labor market.
Recent Trends in Immigration
Partly as a result of changes made in immigration law in the mid-1960s, as well as subsequent changes, the level of immigration has been rising steadily for the last three decades. At present, between 700,000 and 900,000 legal immigrants and an estimated 420,000 illegal immigrants settle permanently in the country each year (Statistical Yearbook of the Immigration and Naturalization Service, 1997). As a result, the immigrant population has grown rapidly, almost tripling in number from 9.6 million in 1970 to 26.5 million by the beginning of 1999, not including the U.S.-born children of recent immigrants.
As the level of immigration has increased over the last three decades, the education level of each new wave of immigrant has declined in comparison to natives (Borjas 1999; Edmonston and Smith, 1997). Because education has become so central to economic well-being in the modern American economy, this decline has prompted many to worry that immigrants may be falling behind natives in a variety of social measures. One of the most worrisome consequences of declining immigrant skills is that a large percentage may end up in jobs that pay poverty-level wages and provide few non-monetary fringe benefits—including health insurance. Under such circumstances a large share of immigrants and their dependents would not only lack employment-based health coverage, they also would find it difficult to purchase it privately given their limited financial resources.
Purpose of Research
The overriding goal of this paper is to help bridge the gap between health insurance and immigration policy circles. As this paper will make clear, the two issues are much more intimately linked than is commonly supposed. To this end we first examine the direct effect immigration has on the size and growth of the uninsured population at the national level, and where possible at the state and local level, using the latest data available. Second, in order to better understand why immigrants and their children lack insurance, this paper provides detailed information on the socio-demographic characteristics of the uninsured based on whether they reside in a native- or immigrant-headed household. It is our hope that this will help to better inform policymakers, researchers, and others interested in the ongoing debate over health care and immigration.
What Does it Mean to be Uninsured?
There are, of course, many different kinds of health insurance. Moreover, tests and procedures covered, drug benefits, ability to choose one’s doctor, deductibles, and total benefit limits vary widely among plans. This paper relies on the definition of insurance used in the Census Bureau publication, Health Insurance Coverage 1998: Current Population Report P60-208. We also use the same data source used in that report, the March 1999 Current Population Survey (CPS) collected by the U.S. Census Bureau. While other data sources are also used, much of the previous research, as well as figures published by the federal government on the uninsured, relies on this definition and data source.1
A person is considered to have health insurance if he or she responds yes to any of a series of questions that ask whether the person was covered by insurance provided by an employer (including insurance provided to military personnel, veterans, and their families), or whether he or she was covered by a family member’s policy, Medicare, Medicaid,1 or insurance purchased by him- or herself during the year prior to the survey. These questions are designed, according to the Census Bureau, to measure whether an individual was without health insurance coverage during the entire calendar year. Based on the March 1999 CPS, persons who responded that they did not have any type of health insurance in the prior year are considered to have been uninsured for all of 1998.
Why Study Immigration’s Impact on the Size of the Uninsured Population?
In any discussion of immigration’s impact on the size of the uninsured population, it is important to keep in mind that immigration is different from other factors that may have contributed to the problem because immigration is a federal policy. The federal government controls both the number of legal immigrants allowed into the country each year and the selection criteria used for admission. Moreover, the federal government determines the level of resources and the tactics devoted to controlling illegal immigration. Thus, the level of immigration and the composition of the immigrant population stems directly from federal policy — a policy that can be altered at any time. Even if it were desirable, the government cannot legislate a pause in the advance of medical technology or easily reduce the strong demand for health care in an aging and increasingly secular society, two factors which have driven up costs. But it can change immigration policy.
One may still reasonably ask if it matters what proportion of persons in immigrant households, or even in native households for that matter, do not have health insurance. What effect, if any, does a lower national or local rate of health insurance coverage have on the country as a whole or in a particular part of the country, especially for the majority of the population who do have health insurance? In addition to altruism, there are a number of very practical reasons to be concerned about the level of insurance coverage in America and the role that immigration policy may be playing in this growing problem.
Impact on The Uninsured Already Here
Probably the most obvious reason for concern is the impact on the uninsured already here, both native and immigrant. The cost of efforts to provide insurance to those without it or to provide basic care if more comprehensive insurance is not provided, depends in large part on the number of people in need of such assistance. If immigration increases the number of people who require government financed or subsidized health care, then the total cost of such efforts must grow accordingly. Increasing the total cost of efforts to provide insurance and health care to the uninsured can only reduce political support for such efforts. Alternately, if federal, state, and local government outlays on programs for the uninsured remain relatively constant, then the level of services provided to each recipient must be reduced. This, too, is clearly not in the interest of America’s uninsured. A large increase in the size of the uninsured may also strain the resources of non-governmental institutions and charities that provide health care to the uninsured, thereby reducing what they can provide to each individual. A recent report from the Institute of Medicine concluded that the financial viability of institutions that provide health care to the uninsured is more at risk today than in the past; partly because of the rising number of uninsured individuals (Lewin and Altman, 2000). Therefore, if one is concerned about the uninsured already here, significantly increasing the size of the uninsured population is clearly counterproductive. This is likely to be the case no matter what solution is favored to deal with the problem.
Effect on Taxpayers
Probably the most self-interested reason to be concerned about a rise in the uninsured population resulting from immigration is its effect on public coffers. The uninsured still become injured or ill and need medical attention. While their options may be more limited, not having health insurance does not mean that uninsured patients receive no medical care. Rather, they often postpone medical attention until their condition has worsened (Budetti et al., 1999). The uninsured seek treatment from "safety net providers," such as public hospitals, community health clinics, and local health departments (Lewin and Altman, 2000; Gage and Regenstein, 1999). Thus, individuals without insurance do receive care, but often it is the most expensive and least efficient means of obtaining treatment.
In many cases, the cost of providing medical services to the uninsured is paid for by federal, state, and local governments. For many counties and cities, the costs of operating a public hospital and/or clinics, which provide much of their services to the uninsured, account for a sizable portion of their total budget. In addition, health care providers are often reimbursed by the federal government for costs incurred in providing care to the uninsured. The amount of public money that goes to provide health care to the uninsured is substantial. Because of the diversity of funding sources, the complex and decentralized way in which they are administrated, and the limited availability of data, no exact estimate exists for the total public cost of providing care to the uninsured. It is likely, however, between $15 and $30 billion per year is spend on the uninsured by government at all levels.3 These costs do not include the more than $150 billion spend annually by the federal government and states to provide Medicaid coverage to low-income residents. Whatever the cost of providing services to those without insurance, there can be no doubt that an increase in the size of the uninsured population resulting from immigration has significant negative implications for taxpayers.
Higher Premiums and Costs for Those with Insurance
While governments at all levels do compensate health care providers for some of the care given to the uninsured, a significant portion of the care is not compensated and must be simply written off by providers as charity because collecting money from the uninsured can be very difficult given their limited financial resources in most cases. (Lewin and Altman, 2000). Hospitals and other health care providers simply cannot absorb all of the costs of providing such charity care and so they pass at least some of the costs along to paying customers in the form of higher prices for treatment, which in turn creates higher insurance premiums for those with insurance. There is evidence, however, that in the new managed-care environment, cost-shifting has become difficult for health care providers, though it is clear that some cost-shifting continues to occur from those with insurance to those without (Morrisey 1996).
For workers whose employers pay for all or almost all of their health care premiums, these costs remain largely hidden (Castro, 1994). But in the long run, the rising costs associated with providing care to the uninsured must make employers increasingly reluctant to offer it or to require employees to pay an ever larger share of the premiums. The higher costs caused by the uninsured may also force some employers with limited financial resources, who wish to continue to provide coverage, to offer smaller wage increases or curtail other fringe benefits so that they can continue to afford higher insurance payments. The situation is even worse for Americans who must purchase their own insurance without the aid of an employer, because they will be forced to bear the costs of higher premiums directly, without an employer to share part of the increase.
In this way a growing uninsured population creates its own momentum by making it more likely that employers will shift the costs of insurance to their employees and by pushing the costs of insurance out of reach for Americans with moderate incomes who must purchase insurance on their own. There can be little doubt that increases in the cost of health insurance can only make it more difficult for employers and low-income Americans to afford health insurance. Thus, while it may appear at first glance that the growth in the uninsured population is of little concern to those who have insurance, this is clearly not the case.
In modern America, at least some services will always be provided to those without insurance, even if the costs of doing so are high. Thus, the size of the uninsured population should be of concern to all members of society because all members will have to pay for these costs through higher taxes, higher premiums, or some combination of the two.
Increasing the Risk for the Spread of Communicable Diseases
In addition to monetary concerns over the costs of the uninsured, there are also very real public health issues associated with a large uninsured population. Because they often do not receive routine preventive care and often seek out medical attention only when their condition is more serious, the uninsured may unintentionally extend the period of time the public is exposed to communicable deceases. This problem is likely to be of particular concern among immigrants because most come from developing countries where communicable diseases are more common. For example, tuberculosis in the United States is disproportionately concentrated in the immigrant population. In 1998, about 42 percent of the 18,361 known cases in the United States were among immigrants (Sachs, 2000). The resurgence of TB, especially strains of the disease that are drug resistant, constitutes a growing health care threat. If many immigrants are uninsured, this may represent a significant impediment to dealing with this problem. At the very least, it is clear that a lack of health insurance among immigrants has important implications for the health of the entire society.
Implications for Immigrant and Immigration Policy
In addition to the impact on native-born Americans, looking at insurance among immigrants and their children is also important because it is one way of evaluating the consequences of current immigration policy. Perhaps most important, it also gives us a good idea of how immigrants admitted in the future are likely to do in the United States if immigration policy remains unchanged. Having health insurance and access to health care is one measure of incorporation and integration in the economic and social mainstream. Low rates of coverage imply that, for whatever reason, a significant proportion of immigrants have not successfully adapted to life in the new country, at least with regard to health insurance. This is particularly important because, without a change in immigration policy, 10 million new immigrants will likely settle permanently in the United States in just the next decade. If current trends continue, immigration may add an additional three to four million people to the ranks of the uninsured over just the next 10 years. Of course, the extent to which persons in immigrant households have health insurance today does not tell us exactly how those admitted in the future will fare. Looking at past immigrants, however, is probably the best means we have of predicting how tomorrow’s immigrants will do if the same selection criteria for admission continue to be used.
In addition to immigration policy, which is concerned with who may come and how many, there is immigrant policy, which deals with how we treat the foreign-born living in United States. Looking at health insurance coverage among immigrants is important because if a large percentage of immigrants and their children already here lack insurance, we need to deal with this problem in a constructive manner, whatever immigration policy is adopted in the future. Such things as tax incentives to employers so that they will provide coverage for employees, increasing immigrant use of government-provided health insurance for which they are eligible but do not use, and efforts to improve the labor market skills of immigrants so that they find jobs that offer insurance may all need to be designed with the intent of addressing the particular needs of immigrants. At the very least, if immigrants and their children now comprise a large share of the uninsured, our efforts to deal with this problem, as well as research on health insurance coverage, must take this new reality into account.
Methods and Data
Definitions and Data Sources
The data for this study come from the March 1999 Current Population Survey (CPS) collected by the Census Bureau. The CPS is used because it is the most recent survey available and is the source of most official government statistics on the uninsured. Moreover, it is one of the best sources of information on persons born outside of the United States—referred to as foreign-born by the Census Bureau.4 Persons not born in the United States, one of its outlying territories, or to U.S. parents living abroad are foreign-born. All persons born in the United States, including the children of illegal aliens, are natives. For the purposes of this paper, foreign-born and immigrant are used synonymously.
As already described, this paper relies on the definition of insurance used in the government’s publication, Health Insurance Coverage 1998: Current Population Report P60-208. Persons are considered to have health insurance if they respond "yes" to any of a series of questions that asks whether they were covered by insurance in the year prior to the survey provided by an employer, family member’s policy, the government, or by insurance they purchase themselves. Since the survey was conducted in March 1999, it measures insurance coverage for 1998. No adjustments of any kind are made to the definition of insurance or the data in this paper. Totals for the uninsured presented here match those published by the Census Bureau.
This paper examines insurance coverage for persons living in immigrant- and native-headed households. Individuals related to the household head by blood, marriage, or adoption, regardless of their own nativity, are considered to be in an immigrant or native household based on whether the household head is foreign-born or a native. Individuals unrelated to the head are considered immigrant or native based on the nativity of the head of the family in which they reside. For example, a foreign-born husband and wife (one of them would be the head) with two young U.S.-born children are counted as a household of four people living in an immigrant household. If the same family were to rent a room to an unrelated native-born woman with a child of her own, then the woman and her child would be counted as a separate native household, even though she and her child live under the same roof as the immigrant family and are technically in the same household as the immigrant family. Persons who live by themselves or with others to whom they are unrelated are, in effect, their own households and are considered immigrant or native based on their own nativity. Households are defined in this way so that they more accurately reflect the kind of income sharing and insurance eligibility that exists among members of the same family. Its worth noting that individuals unrelated to the household head only comprise about 4 percent of the population, therefore how they are allocated does not substantially affect the results.
Composition of Immigrant Households
Using the above definition, 92.4 percent of the people living in immigrant-headed households were immigrants themselves (67.3 percent) or the native-born child under age 21 (25.1 percent) of an immigrant father or mother based on the March 1999 CPS. In households headed by immigrants who arrived after 1970, 96.3 percent of the people are either immigrants or their U.S.-born children under the age of 21. Therefore, this approach primarily measures insurance coverage for immigrants and their children. Since a child’s standard of living, including access to health insurance, is a function of his parents’ income, this method captures the full effect of immigration on the size of the uninsured population in the United States. Unless otherwise indicated, country of origin and year of entry for immigrant households are based on the responses of the household head.
Findings
High Percentage of Persons in Immigrant Households Lack Insurance
Figure 1 shows the proportion of persons in immigrant- and native-headed households who have no health insurance, also referred as the uninsured. Figure 1 also shows the percentage who are covered by Medicaid, the means-tested health insurance program provided by the federal government and states. (The figures for Medicaid include persons using the Indian Health Service as well as state programs, such as California’s Medi-Cal). In 1998, 32.4 percent of all persons in immigrant households were without health insurance. This was more than twice the rate for persons in native households — 13.9 percent of whom lacked health insurance. This means that, astonishingly, nearly one out of three persons in immigrant households had no health insurance in 1998. The difference in rates of insurance coverage is statistically significant using either a 90 percent or 95 percent confidence level. This means that we can say with 95 percent certainty that the gap in rates of insurance coverage in the CPS represents a real difference in the actual population.
Compared to other subgroups in the population, the percentage of persons without health insurance in immigrant households is extremely high. Even in comparison to groups that traditionally have a high percentage without insurance, the rate for those in immigrant households stands out. For example, it exceeds the rate for African-Americans, 22.2 percent of whom lack insurance, and also exceeds the rate for high school dropouts,5 26.7 of whom lack insurance, and it is about equal to the 32.3 percent of all persons living in poverty who are uninsured. If many observers have described the fact that 16.3 percent of the nation’s total population lacks insurance as a severe problem, then the situation for immigrants and their children can only be described as a crisis.
Immigrant Households Account for a Large Share of Uninsured Population
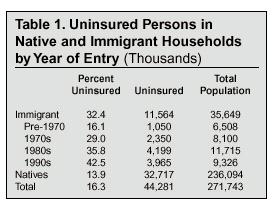
The high percentage of persons in immigrant households without insurance coupled with the very large number of people living in immigrant households means that immigration has had a very significant effect on the overall size of the uninsured population. Table 1 provides percentages and totals for persons without health insurance living in immigrant and native households. In 1998, persons in immigrant households accounted for 26.1 percent or 11.6 million of the 44.3 million people in the United States who lacked health insurance. Since persons in immigrant households account for only 13.1 percent of the country’s total population, their disproportionate representation among the uninsured reflects the very high percentage who do not have health insurance. Put another way, the uninsured population is one-third larger (32.7 million versus 44.3 million) because of immigration. Clearly, the impact of immigration on the health insurance problem in the United States is difficult to overstate.
Welfare Reform is Not to Blame
In 1996, concern over immigrant use of means-tested programs led Congress to reduce welfare eligibility for some immigrants as part of a general overhaul of the welfare system. In particular, Congress made some recent non-humanitarian immigrants (i.e., not refugees and asylees) ineligible to receive several federally funded programs, including SSI, AFDC/TANF, and food stamps, until they had been in the country for a certain period of time. Since persons receiving cash assistance programs like SSI and AFDC/TANF are automatically eligible for Medicaid coverage, changes in immigrant eligibility for these programs might explain why so many persons in immigrant households do not have health insurance. The available evidence, however, indicates that this is clearly not the case. Lack of insurance coverage was a severe problem for persons in immigrant households before welfare reform. In 1995, 30.5 percent of persons in immigrant households were uninsured.6 This is very similar to the 32.4 percent who were uninsured in 1998. Moreover, the gap between persons in immigrant and native households has remained roughly the same size since 1995. In that year, 13.2 percent of persons in native households lacked health insurance, so there was a 17.3 percentage point gap between immigrant and native households. This is only slightly smaller than the 18.5 percentage point gap that existed in 1998 between the two groups. It is true that Medicaid use among persons in immigrant households has fallen significantly since 1995, but it has also fallen sharply for persons in native households. Between 1995 and 1998, Medicaid use declined 15 percent for persons in native households and a little less than 18 percent for persons in immigrant households. As Figure 1 shows, despite falling Medicaid use, persons in immigrant households are still significantly more likely to be on Medicaid than those in native-headed households.7 In 1998, 13.8 percent of persons in immigrant households used Medicaid compared to 9.7 percent of people in native households. Since the percentage of persons in immigrant households on Medicaid remains higher than that of persons in native households, it is hard to argue that low rates of Medicaid use alone account for the higher percentage of immigrants and their children who are uninsured.
The fact that welfare reform does not explain the lack of insurance coverage for persons in immigrant households does not mean that Congress was right to curtail welfare eligibility for immigrants. As we will see, the low level of educational attainment and high poverty rates of many immigrants and their children indicates that they need access to the welfare system even more than do natives. While it may make little sense to have an immigration policy that admits large numbers of people who end up in or near poverty and need to use means-tested programs, cutting welfare benefits to immigrants after they have already been allowed into the country seems neither fair nor wise.
Recent Immigration Accounts for Much of Growth in the Uninsured Population
One of the reasons policymakers, politicians, the media, and researchers have devoted so much attention to the uninsured population is that it has grown significantly in recent years. As previously discussed, both the percentage of the population without health insurance and the size of the uninsured population have grown significantly in recent years. The growth in the uninsured population continued through the 1990s, despite a strong economy over most of the decade. What has not been generally acknowledged is that much of this increase was caused by newly arrived immigrants and their children. The Current Population Survey asks immigrants when they came to the United States. therefore, it is possible to estimate the direct impact of recent immigration on the size of the uninsured population. In 1998, 2.58 million of the 5.32 million immigrants who indicated that they had arrived between 1994 and 1998 lacked health insurance. In addition, 114,000 of the 424,000 children born in the United States to immigrants that arrived in this time period also lacked health insurance.8 This means immigration accounted for 2.7 million or an astonishing 59 percent of the 4.67 million increase in the size of the uninsured population that took place after 1993. Looked at from a different point of view, if all persons in immigrant households are excluded from the data, the percentage of the population without health insurance in the United States would be 13.9 percent (the current rate for persons in native households and the national rate back in 1990). These numbers indicate that immigration policy has become central to an understanding of the growing health care insurance crisis in the United States. Without immigration, the size and scope of the problem would be significantly different.
Lack of Insurance Remains a Problem Even After Many Years in the Country
While recent immigrants and their children account for much of the recent growth in the uninsured population, this would not be as much a matter of a concern if immigrants obtained insurance soon after arriving in the country. In addition to overall totals, Table 1 reports the percentage of persons who lack health insurance based on the year of entry of the household head. Looking at insurance coverage by entering cohort is useful because it is one of the best ways of determining the progress of immigrants over time. Table 1 shows that the longer immigrants reside in the United States, the more likely they are to have health insurance. This is certainly to be expected. As immigrants become more familiar with their new country and as their work experience grows, their access to health insurance increases. However, the table also shows that even after immigrants have been in the country for a long period of time, the percentage without health insurance remains extremely high. For example, 35.8 percent of persons living in households headed by an immigrant who arrived in the 1980s still did not have insurance in 1998, even though in most cases the household head had been in the country for 10 or more years. Turning to persons living in households headed by immigrants who arrived in the 1970s, 29 percent were without coverage, even though most of the heads of these households had been in the country for more than 20 years. With the exception of pre-1970 immigrant households, the differences between persons in immigrant and native households by year of entry is statistically significant. The higher rates of insurance coverage of pre-1970 immigrants may partly reflect the fact that most of these immigrants were admitted under the system that existed prior to 1965, which tended to produce a more educated flow of immigrants. The results in Table 1 make clear that although the percentage without insurance does decline over time, many persons in immigrant households do not acquire insurance even after they have been in the country for many years.
The figures in Table 1 report insurance coverage for all persons in immigrant households. One might assume that the immigrant themselves have much higher rates of insurance coverage, but that it is their dependents who are often without insurance. Analysis of only immigrants, however, indicates that this does not appear to be the case. In 1998, 27.2 percent of immigrants who arrived in the 1970s were without insurance; for 1980s immigrants, the figure was 37 percent and for immigrants who arrived in the 1990s, 47.2 percent lacked insurance. While these percentages differ somewhat from those in Table 1, the same basic pattern remains. Even after they have lived in the United States for many years, lack of insurance coverage among immigrants is very common. These findings indicate that despite generally favorable economic conditions over the last two decades, many immigrants are unable or are unwilling to acquire health insurance. Even 1970s immigrants are twice as likely as natives to be uninsured. The fact that such a high percentage of established immigrants do not have insurance raises the question of whether low rates of insurance coverage, at least to some extent, reflect a choice on the part of some immigrants, rather than economic necessity. This issue will be explored later in this report.
Majority in Immigrant Households Without Insurance Are Legal Residents
While Table 1 indicates that persons in immigrant households make up a large share of the uninsured, it does not provide information about their legal status. It is possible that illegal aliens (also called undocumented or unauthorized immigrants) account for a large percentage of persons in immigrant households without insurance. Knowing the legal status of those who lack insurance may be important because it provides useful information about the extent to which the problem is explained by the presences of illegal immigrants in the country. While it is not possible to definitely identify illegal aliens in the CPS, it is possible to estimate their number and their rate of insurance coverage. Research by Clark and Passel (1998) and Warren (1999) indicates that five million illegal aliens were counted in the March 1999 CPS.9 To estimate the percentage who lack insurance, it is possible to use persons with demographic characteristics that are thought to be similar to those of illegal aliens. This paper uses immigrants who are not citizens; who lack a college education; who are under age 65; who are from Mexico, the Caribbean (excluding Cuba), and Central America; and who arrived between 1986 and 1998 as representative of illegal aliens. In the March 1999 CPS, the percentage of these individuals who lacked insurance was very high — 63.9 percent. To calculate the impact of illegal aliens on the size of the uninsured population, we assume that the same percentage of illegals (96.9 percent) live in immigrant households as our surrogate population. If the rate of insurance coverage and distribution across households is the same for illegal aliens as for this surrogate population, then 3,095,955 or 26.8 percent of the 11,564,000 people without insurance living in immigrant households are in the country illegally. Alternately, 73.2 percent or 8,468,045 of persons in immigrant households were legal immigrants or the U.S.-born children of immigrants. These results also imply that 27.5 percent of persons in immigrant households who reside in the country legally are without health insurance. While this is somewhat lower than the 32.4 percent for all persons in immigrant households when illegal aliens are included, it is still dramatically higher than the 13.9 percent for persons in native households. Clearly, these estimates indicate that illegal aliens contribute significantly to the problem. However, they also indicate that illegals account for only about one quarter of persons in immigrants households who do not have insurance. Even when illegals are excluded, the 27.5 percent of persons in immigrant households who are without insurance is still about twice the rate for individuals in native households.
The estimates provided above probably overstate the impact of illegal immigration for two reasons. First, defining who is an illegal alien is not as straightforward as it might seem. A large percentage of those in the country "illegally" actually have the permission of the federal government. Many are asylum applicants awaiting the outcome of their petition to stay in the country. Others enjoy temporary protected status (TPS) because, although they do not qualify for political asylum, the federal government will not deport them or require them to leave because it is thought conditions in their home countries are too unstable or chaotic for them to return. In addition, there are still several hundred thousand persons who are the spouses and children of amnesty beneficiaries from the 1980s who are also allowed to stay in the country. If all of these "semi-legal" immigrants are excluded, illegal aliens would account for an even smaller share of those without insurance living in immigrant households.
The second reason that the estimated impact of illegal aliens may be overstated in the above calculations is conceptual. It may make more sense when evaluating the impact of immigration to view legal and illegal immigration as closely linked and not as distinct phenomena. Many illegal aliens come to the United States to join friends and family members who are legal residents. Sociological research indicates that one of the primary factors influencing a person’s decision to emigrate is whether a family member or person from their home community has already come to United States (Massey and Espinosa 1997; Palloni, Spittel, and Ceballos 1999). Communities of recent legal immigrants serve as magnets for illegal immigration by providing housing, jobs, and entree to America. The close link between legal and illegal immigration can also be seen in analysis done by the Congressional Research Service that estimates that one out of four legal immigrants who receives a green card in any given year is in fact an illegal alien already living in the country (Cited in Vaughan,1997). Thus, it is probably more accurate to view illegal immigration as a direct consequence of large-scale legal immigration and not as a separate phenomenon. If this is correct, it makes more sense to look at the characteristics of all immigrants as reflective of the nation’s immigration policy in its totality, not to separate out illegal aliens from legal immigrants.
Socio-Demographic Characteristic
Insurance Coverage by Educational Attainment
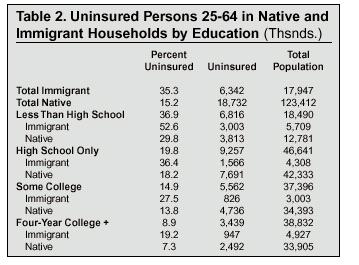
One of the best predictors of the propensity to have insurance is a person’s education level, regardless of nativity or income. This is true for several reasons. First, because of the limited value of their labor in an economy that increasingly demands more skilled workers, those with little education are the most likely to hold jobs that do not offer health insurance as a fringe benefit or, if insurance is offered, the workers must pay a large share of the costs. Second, those with little education have the lowest incomes and may find it very difficult or simply impossible to afford to insurance on their own. Third, persons with few years of education have the most unstable employment histories—suffering higher unemployment rates and longer periods of unemployment than educated workers whose skills are more in demand. Since loss of insurance often accompanies loss of employment, higher rates of unemployment should have an effect on rates of insurance coverage. Table 2 reports the health insurance coverage of persons between 25 and 64 years of age in immigrant and native households by educational attainment. The table indicates that insurance coverage varies enormously based on education level, regardless of nativity. In 1998, 36.9 percent of all dropouts were without insurance; for persons with only a high school education, 19.8 percent were uninsured; for those with some college, 14.9 percent had no insurance; and 8.9 percent of individuals with four years of college were without health insurance. Since persons aged 25 to 64 in immigrant households are much more likely than those in native households to lack a high school education (31.8 percent compared to 10.4 percent), the high percentage of persons in immigrant households who have no insurance is at least partly explained by the higher proportion with few years of schooling.
Table 2 also shows, however, that education alone does not account for the lower rate of insurance coverage associated with immigrants. At every education level, adults in immigrant households are twice as likely as adults in native households to lack insurance. Thus, a lower level of education is by no means the only factor accounting for the high percentage of persons in immigrant households who lack insurance.
One way of examining the importance of education in explaining the lack of insurance associated with immigrants is to calculate the rate of coverage for persons 25 to 64 in immigrant households, assuming that their educational endowment was the same as persons in native households. In other words, what percentage of working age adults in immigrant households would lack insurance if their distribution across educational categories was the same as persons in native households and their rate of insurance coverage by education was unaltered. In 1998, if persons in immigrants households had the same educational endowment as natives, but retained the same rates of coverage by educational category, 30.9 percent of persons in immigrant households would have been without insurance. While this is less than the actual 35.3 percent who lacked insurance in 1998, it is still dramatically higher than the 15.2 percent for working-age adults in native households. This suggests that 4.4 percentage points or 22 percent of the 20.1 percentage point gap in the insurance coverage for persons 25 to 64 in immigrant and native households is accounted for by the lower levels of education associated with immigrants. While these results indicate that education is clearly an important factor, the causes of the problem are more complex. Other factors must also contribute significantly to the lack of insurance for individuals in immigrant households.
Insurance Coverage by Age
In addition to education, age also has an impact on one’s likelihood of having health insurance. Table 3 reports health insurance statistics by age for persons in immigrant and native households. As the table indicates, insurance coverage is less common among those 18 to 64 than for both children and older people. Most persons over 65 have insurance because all persons who receive Social Security, or who have a spouse who receives Social Security, automatically qualify for Medicare. While a larger share of persons in native households are over age 65 (12.5 percent compared to 7.9 percent for immigrants), this does not explain the difference in rates of insurance coverage between immigrant and native households. Even when retired persons are excluded, the gap between immigrants and natives remains.
Turning to children (17 and under) first, we see that overall they have a somewhat higher rate of insurance coverage than adults because children in low-income families are often eligible for government-provided means-tested insurance even when their parent are not. Since 1997, the federal government, along with the states, has had some success in increasing insurance coverage among children in low-income families under the State Children Health Insurance Program or SCHIP (Morse, 2000). Even so, about one in seven children in the United States was without health insurance in 1998.
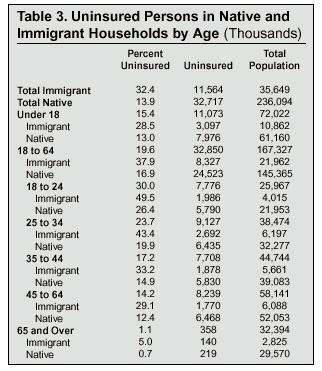
Table 3 shows that children in immigrant households have much lower rates of insurance coverage than do their counterparts in native households. In 1998, 28.5 percent of children in immigrant households were without health insurance, compared to 13 percent in native households. The 3.1 million children in immigrant households who lack insurance now represent 28 percent of all uninsured children. There can be little doubt that recent immigration is making it more difficult and costly to reduce the number of children without insurance under SCHIP. Congress passed SCHIP in 1997 in an effort to increase insurance coverage among low-income children and it is expected to cost the federal government $20 billion over five years. By April of 2000, an estimated one million eligible children have been provided insurance as part of SCHIP (Morse, 2000). But immigration certainly has the potential to undo much of that progress. In 1998 there were 588,000 immigrants under the age of 19 (SCHIP’s target population) without insurance who had arrived in just the last four years. In addition, there were 114,000 children born to adult immigrants who arrived during the same period who did not have insurance in 1998. Thus, because of recent immigration the number of children without health insurance was more than 700,000 larger than it would otherwise have been, erasing most of the gains made so far under SCHIP. In the years to come, it is very likely that immigration may offset much of the progress made as a result of SCHIP
While the gap between children in immigrant and native households is very large, it is also extremely large for persons between the ages of 18 and 64 and for all subdivisions of that age group. Table 3 indicates that 37.9 percent of individuals in immigrant households between 18 and 64 lacked insurance in 1998, compared 16.9 percent of individuals in native households. This difference can only be described as huge, with those in immigrant households being more than twice as likely to lack insurance as those in native households. Table 3 also shows that differences in the age distribution between persons in immigrant and native households do not account for the dramatically lower rates of insurance coverage associated with immigrants. In some of the younger age groups, the gap between persons in immigrant and native households is actually larger than the gap among all persons in immigrant households and all persons in immigrant households. For example, there is a 23.1 percentage point gap between persons aged 18 to 24 in immigrant and native households. This difference is slightly larger than the 18.5 percentage point gap that exists when comparing all persons in immigrant households to all persons in native households. Therefore, the age distribution of persons in immigrant households would seem to account for little if any of the large difference between the two groups in insurance coverage. We must look elsewhere if we are to understand why so many immigrants and their children lack health insurance.
Insurance Coverage by Country and Region of Birth
Table 4 reports insurance coverage by regions of the world and country of birth based on the household head. Turning to region of birth first, the table reveals that while persons in immigrant households are much more likely to be without insurance than those in native households, there are substantial differences among immigrants. Persons in Mexican- and Central and South American-headed households are the most likely to lack health insurance. In contrast, households headed by Canadian and European immigrants are the most likely to have health insurance. The sizes of the differences between regions are very large in some cases. Persons in Mexican and Central American households, for example, are more than three times as likely to be uninsured as persons in households headed by immigrants from Europe and Canada.
While there are some immigrant groups who are about as likely as natives to have insurance, lack of health insurance coverage is widespread among immigrants and is not simply confined to a few groups. In addition to the very large share of persons in Mexican and Cental American households without insurance, persons in households headed by immigrants from Sub-Saharan Africa, the Middle East, South Asia, South America and the Caribbean are either twice as likely to be without insurance as are persons in native households or very nearly so. While it is clear that lack of health insurance is a much greater problem for some groups than others, low rates of insurance coverage is common among many immigrant groups.
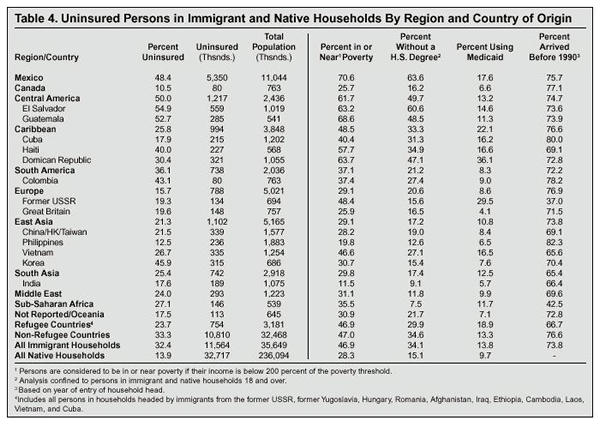
In addition to insurance coverage by region of origin, Table 4 also reports the percentage uninsured for the 15 countries with the largest number of post-1970 immigrants living in the United States in 1998. Given the sample size of immigrants from some countries, however, the differences between countries should be interpreted with caution. Smaller sample size means that there is greater variability for individual country estimates than for the estimates based on region of origin. The estimates for individual countries should be used to make determinations of the relative differences between countries, and should not be seen as quantified absolute differences. Table 4 shows that like the data by region, rates of insurance coverage differ significantly by country. In fact, the variation between immigrant households from different countries is much larger than is the difference between persons in immigrant and native households. In 1998 for example, the percentage of persons without insurance in Salvadoran households was more than five times that of persons living in households headed by Canadian immigrants. Even among immigrants from the same region of the world, rates of insurance coverage vary significantly. For example, persons in Korean households are much more likely to be uninsured than immigrants from other East Asian countries. Among Caribbean immigrants, persons in Cuban household are much more likely to be uninsured than are persons in households headed by immigrants from that region.
What Accounts for the Large Differences Between Immigrant Groups?
While Table 4 is not a fully developed explanatory model of insurance coverage, it does provide important clues to why there are such large differences between immigrant groups. The right side of the table reports different characteristics for persons in immigrant households by region and country of origin. The first column on the right-hand side reports the percentage of persons who are in or near poverty using the official federal threshold.10 Groups, such as Mexicans, Central Americans, and those from the Caribbean, who have the highest poverty rates, also tend to have the lowest rates of insurance coverage. The same is true for education levels, which is reported in the second column on the right. A large share of adults in households headed by immigrants from these regions lacks even a high school education. Of course, high poverty rates and low levels of education do not explain all of the differences. Persons living in Dominican-headed households, for instance, are much more likely to be insured, despite very high poverty rates, than persons living in Mexican or Central American households. The main reason Dominicans are more likely to have insurance is that they make use of Medicaid at much higher rates than do other groups. It would appear that high rates of Medicaid use can offset, at least in part, the very low incomes of many Dominican households. Another example of Medicaid offsetting higher poverty rates can be found among households headed by immigrants from the former Soviet Union. While their poverty rates are high, their very heavy use of the Medicaid system means that the percentage without insurance is relatively low. The last column in the table shows the percentage of persons living in households headed by pre-1990 immigrants. One would expect that those groups that have been in the country longer on average would be the most likely to have insurance. While there is some evidence for this in the table, the relationship between insurance coverage and duration of stay seems weaker than for the other causal factors reported in the table. Of course, it should be recalled from Table 1 that lack of insurance remains a severe problem even after immigrants and their children have been in the country for many years. Therefore, it is not surprising that the percentage of persons living in established households seems to account for little of the difference between immigrant groups.
Insurance Coverage for Refugees and Asylees
The bottom portion of Table 4 gives estimates of insurance coverage for immigrants from the major refugee-sending countries. Not all individuals from these countries were admitted as refugees, but by reporting estimates separately for persons in households headed by immigrants from these countries, it is possible to gain some insight into the extent to which the lack of insurance coverage for persons in immigrant households reflects immigrants admitted based on humanitarian criteria. The table shows that immigrants from these countries are actually less likely to be uninsured than immigrants from non-refugee countries. In 1998, 23.7 percent of people living in households headed by an immigrant from one of the major refugee-sending countries were uninsured, compared to 33.3 for persons in household headed by immigrants from non-refuge-sending countries. The table also shows that, not surprisingly, persons in households headed by immigrants from refugee countries have much higher rates of Medicaid use than do other immigrants. In fact, the rules governing use of the entire welfare system (including Medicaid) by immigrants admitted for humanitarian reasons are more generous than for non-humanitarian immigrants and even for natives. As a result, the percentage without insurance in refugee households is somewhat lower than for other immigrants. While Table 4 does not definitively identify refugees, one thing is clear from these estimates: The high percentage of persons without health insurance in immigrant households is not a function of humanitarian immigration. Persons in immigrant-headed households headed by immigrants from non-refugee countries are much more likely to be uninsured than are those in households headed by immigrants admitted for humanitarian reasons.
Insurance Coverage by Race
Race is also an important predictor of insurance coverage. Table 5 reports health insurance statistics by race for persons in immigrant and native households, with Hispanics treated as a separate and discrete category. Since region of the world is closely correlated with race, the pattern in Table 4 follows the same general pattern found in Table 5. White and Asian immigrant households are the most likely to have insurance, while Hispanic and black immigrant households are the most likely to be without insurance coverage. Table 5 shows that immigrant households have a very large impact on the overall rate of insurance coverage for all Hispanics and Asians. In 1998, 20.7 percent of all Asians were uninsured—6.8 percentage points higher than natives. However, when only Asians living in households headed by a native are examined, the rate is 14.4, roughly the same as the 13.9 percent for all natives. Persons in immigrant households also have a significant effect on the rate of insurance coverage for Hispanics. In 1998, 35.3 percent of all Hispanics were uninsured. For Hispanics in native households the rate was 24.8, 10 percentage points lower than for all Hispanics, and 20 points lower than Hispanics living in a households headed by an immigrant. These data indicates that immigrants and their children have a very large impact on rates of insurance coverage for some racial minorities. This strongly suggests that what could be interpreted only as reflective of racial disparities in the United States may in part actually reflect immigration policy.
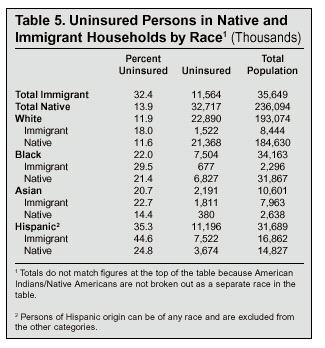
Income, Poverty Status, Workforce Status, and Employer Size
This section examines health insurance coverage for persons in immigrant and native households based on their economic characteristics. As we will see, having health insurance is correlated with other measures of economic welling-being. In the analysis that follows, we further develop the relationship between insurance and such factors as income and work force status.
Insurance Coverage by Income
Table 6 shows health insurance coverage for persons in immigrant and native households by annual household income.11 It shows that there is a strong positive relationship between income and health insurance coverage. Persons with low incomes are the most likely to lack insurance, while those with the highest are the most likely to have insurance. In 1998, 27.0 percent of all persons in households with incomes of less than $25,000 were without insurance compared to 7.3 percent of all persons in households with incomes of $75,000 a year or more. Since 36.3 percent of persons in immigrant households (compared to 27.5 percent of natives) live in households with incomes below $25,000, it is not surprising that immigrants and their dependents are much more likely to be uninsured. Moreover, only 18.5 percent of persons in immigrant households had incomes of more than $75,000 a year, compared to 23.8 percent of persons in native households. Their higher concentration at the bottom of the income distribution as well as their under-representation at the top of the income distribution accounts for some of the large difference in insurance coverage between immigrant and native households.
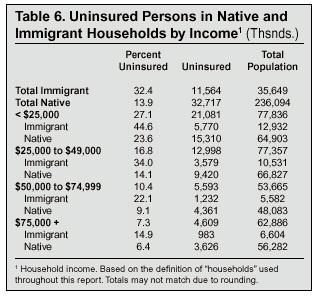
However, Table 6 also shows that persons in immigrant households are still much more likely than those in native households to lack insurance even after controlling for income. In every income category in Table 6, the gap in insurance coverage between the two groups is dramatic. At the bottom of the income distribution (<$25,000) for example, persons in immigrant households are nearly twice as likely to be uninsured as persons in native households with the same income. And for the other three income categories, the percentage uninsured in immigrant households is more than double that of persons in native households. Even among those with incomes of at least $75,000, the difference between persons in immigrant and native households is very large. In fact, the percentage of persons in immigrant households with incomes of over $75,000 who are uninsured is actually slightly higher than for all persons in native households— even though only about one in four people in native households lives in a household with an income that high. In 1998, 14.9 percent of persons in immigrant households with incomes over $75,000 were without insurance, compared to 13.9 percent of all persons in native households. The large percentage of high income immigrants without insurance is striking because even if an employer does not provide any assistance in paying for insurance, households with incomes of more than $75,000 should have the resources to purchase it on their own. Moreover, using the definition of households in this study, immigrant households with high incomes are not much larger than those of natives — both have fewer than four people in them on average. The fact that so many persons in high income immigrant households do not have insurance strongly suggests that this may be a conscious choice on the part of many immigrants, perhaps reflecting cultural attitudes about the value of insurance, rather than an inability to afford coverage.
Insurance Coverage by Poverty Status
It is well established that persons in poverty (also referred to as poor) are at the highest risk for being uninsured (Campbell, 1999). They are often uninsured because many do not work or, if they are employed, work at low-wage jobs that do not provide insurance coverage. Moreover, buying insurance on their own is likely to be very difficult for those in poverty because of their limited incomes. Of course, in many cases persons in poverty are eligible for Medicaid and this tends to increase their rate of insurance coverage. Those with income only just above the poverty threshold (referred to here as the near-poor) also tend to be without insurance for many of the same reasons as those below the poverty threshold.
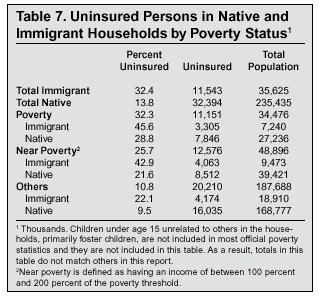
Table 7 reports health insurance coverage by poverty status using the official government poverty threshold. (For a family of four in 1998, poverty was defined as having an income below $16,660.) The table shows that nearly one in three of all persons in poverty lacked health insurance in 1998. However, among the poor there are significant differences between immigrant and native households. In 1998, 28.8 percent of poor persons in native households were uninsured compared to 45.6 percent of persons in immigrants households. The same general pattern exists for the near-poor. Persons are considered to be near-poor in Table 7 if their income is between 100 percent and 200 percent of the poverty threshold—$33,320 for a family of four. In 1998, 42.9 percent of the near-poor in immigrant households were uninsured compared to 21.6 percent in native households. One relatively minor reason persons in immigrant households living in or near poverty are more likely to be uninsured is that Medicaid use among the poor and near poor in immigrant households is somewhat lower than for persons in native households. In 1998, 26.8 percent of persons in native households in or near poverty used Medicaid. In contrast, 24.3 percent of the poor and near poor in immigrant households used Medicaid. However, this small difference only accounts for a small part of the gap between the two groups. If people in immigrant households living in or near poverty used Medicaid at the same rate as their native-born counterparts, 42.2 percent would still be uninsured. While this is lower than the 44.1 percent who were actually uninsured in 1998, it is still much higher than the 24.5 percent of the poor and the near-poor in native household without insurance.
More important than Medicaid use in explaining the lack of insurance coverage associated with immigrants is the fact that persons in immigrant households are much more likely to be in or near poverty than natives. In 1998, more than 20 percent of persons in immigrant households were in poverty in contrast to less than 12 percent of persons in native households. Persons in immigrant households are also more likely to be near-poor than persons in native households—26.6 percent compared to 16.7 percent. Overall, the poor or near-poor accounted for 63.8 percent of the uninsured population living in immigrant households. Therefore, the higher rate of poverty and near poverty is one of the most important reasons why so many immigrants and their children lack insurance. If so many persons in immigrant households were not in or near poverty, the difference in rates of health insurance coverage between individuals in immigrant and native households would not be as large. However, as is the case with the factors examined so far in this report such as education and income, even after accounting for poverty status, immigrants and their children are significantly more likely to be without insurance than similarly situated natives and their children.
Insurance Coverage by Workforce Status
Since most Americans receive insurance through their employers, persons under the age of 65 who do not work tend to have a very low rate of insurance coverage compared to workers. Table 8 reports insurance coverage for persons aged 25 to 64 based on whether they worked in 1998 and, if they did work, whether they were employed full or part time. (Persons are considered full-time if they usually work at least 35 hours per week.) The table shows that 44.4 percent of persons in immigrant households who did not work were uninsured in 1998, compared to 21.7 percent of non-workers in native households. Thus, adults in immigrant households who did not work were about twice as likely to be uninsured as non-workers in native households. This huge difference is striking because by examining only persons in their primary working years, Table 8 does not include the large number of elderly natives who do not work but are covered by Medicare. Moreover, by excluding persons younger than 25 and older than 64, the table compares persons of very similar ages. Persons in this age group in immigrant households are on average 41 years of age while the average for those in native households is 43. This small difference in age cannot account for the huge difference in insurance coverage between the two groups.
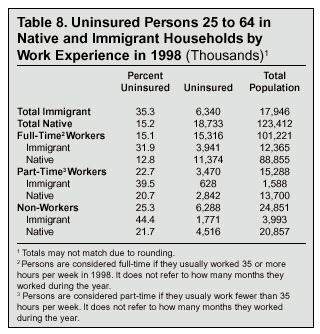
Large differences also exist in insurance coverage for immigrant and native households when we examine full- and part-time workers separately. In 1998, 39.5 percent of persons in immigrant households employed part time were uninsured, compared to 20.7 percent of part-time workers in native households. Turning to full-time workers, the gap is also very large, with 31.9 percent of persons in immigrant households being uninsured compared to only 12.8 percent of persons in native households. This means that persons in native households working part time are much more likely to be covered by health insurance than are full-time workers in immigrant households. This is surprising because full-time workers are more likely to be offered insurance by their employers.
Part of the explanation for the huge difference in insurance coverage is accounted for by the large share of immigrants who hold low-skilled jobs. As shown in Table 2, a much larger share of working-age immigrants have few years of schooling. Because of the limited value of their labor, less-skilled workers often are not offered health insurance as a fringe benefit, or if insurance is offered the employee must pay a large percentage of the costs. However, even when we account for education and confine our analysis to only full-time workers aged 25 to 64, very large differences remain. In 1998 for example, 14.5 percent of full-time workers aged 25 to 64 with at least a four-year college degree in immigrant households were uninsured. In contrast, only 5.9 percent of such persons in native households were uninsured. As we will see later in this paper (Table 10), similar differences exist for other educational categories.
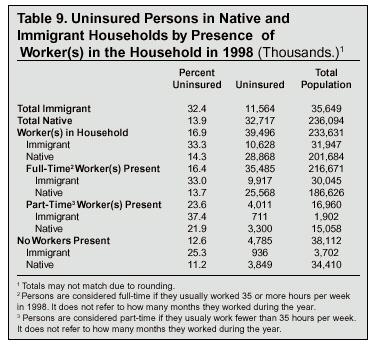
The large differences in rates of insurance coverage between workers in immigrant and native households have important implications not only for individual workers, but also for their dependents. Most children are covered by insurance provided by an employer to their parents and many adults are covered by a spouse’s insurance. Table 9 reports insurance coverage for all persons based on whether there is at least one full- or part-time worker in the household. It shows that persons in households where no one works are the most likely to be insured. At first glance this may seem surprising, until one considers that the vast majority of these individuals are either elderly and covered by Medicare or are welfare recipients and covered by Medicaid. Thus, most of the people in households where no one works do have health insurance.
Table 9 also shows that the vast majority of the uninsured (immigrant and native) live in households with at least one worker.12 In 1998, 91.1 percent or 10.3 million of the 11.6 million of the uninsured in immigrant households lived in a households where at least one person worked. In comparison, a slightly lower percentage (88.2 percent) of the uninsured in native households lived in a household with a least one worker. While the majority of the uninsured live in households with at least one worker, there is stark difference in rates of insurance coverage between immigrant and native households with workers.
One third of persons in immigrant households with at least one worker were uninsured in 1998, compared to 14.3 percent of persons in native households with at least one full-time or part-time worker. The gap in insurance coverage for all persons in immigrant and native households is just as large when we turn to households where at least one of the workers is employed full time. In 1998, 33 percent of persons in immigrant households where there was at least one full-time worker present were uninsured, compared to 13.7 percent of persons in native households with at least one full-time worker. This 19.3 point gap is basically the same size as the 18.5 point difference that exists for all persons in immigrant and native households. The gap is also very large for households with only part-time worker(s), with 37.4 percent of persons in immigrant households lacking insurance in contrast to 21.9 percent of persons in native households. Overall the findings in Tables 8 and 9 indicate that work force experience in 1998 accounts for little of the difference in insurance coverage between the two groups. While the vast majority of the uninsured live in households with at least one worker, the differences in insurance coverage between persons in immigrant and native households can only be described as huge even after controlling for the presence of a worker(s) and the full/part time status of the worker(s).
Insurance Coverage by Employer Size and Education
Table 10 accounts for several factors at once. The table looks at only full-time workers between the ages of 25 and 64, and controls for both education and employer size. This last factor is especially important because smaller firms are less likely to offer insurance to their workers than larger firms. In 1998, only 29.3 percent of all persons working for companies with fewer than 25 employees were covered by insurance provided by their employer. In contrast, two-thirds of those working for employers with more than 500 employees had employer-based health insurance13 (Campbell, 1999). By confining our analysis to full-time workers between the ages of 25 and 64, Table 10 also accounts for both hours worked and age. Because only full-time workers are examined and the age range is limited, the average age for workers in immigrant households is 40 years compared to 41.6 years for those in native households. Thus, Table 10 compares workers of very similar characteristics.
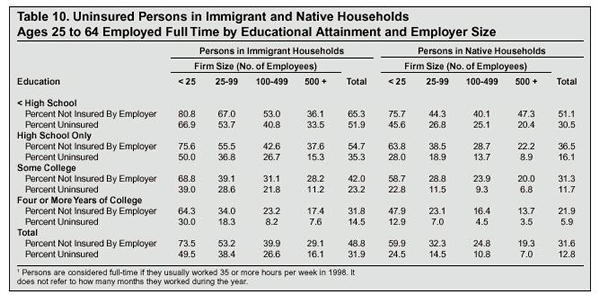
The top portion of each cell in Table 10 reports the percentage of workers in each category who do not have health insurance provided by their employer. Many individuals who do not have insurance through their employer are instead covered by health insurance as part of a family member’s plan or have insurance they purchased on their own. Additionally, in some cases low-wage workers are eligible for insurance provided by the government though Medicaid and some individuals receive insurance coverage because of prior military service. Therefore, the second number in each cell reports the percentage of persons who have no insurance of any kind. Looking at the first cell in the upper left hand corner, Table 10 reads as follows: in 1998, 80.8 percent of full-time workers in immigrant households without a high school degree were not covered by insurance provided by an employer, and 66.9 percent of these same individuals where uninsured. This means that the overwhelming majority of dropouts in immigrant households working full time for small firms were not covered by employer-provided health insurance and were also unable to secure insurance by other means.
Turning next to the totals at the bottom of the table, we find that workers employed at smaller firms are the most likely not to be covered by employer-provided insurance. This is true for both persons in immigrant and native households. For all workers in immigrant households employed at firms with fewer than 25 employees, 73.5 percent did not have employer-provided health insurance and 59.9 percent of all workers in native households working for small firms did not receive insurance from their employers. In contrast, 29.1 percent of all workers in immigrant households employed by a firm with at least 500 employees lacked employer-provided health insurance and for those in native households working for large firms, 19.3 percent did not have health insurance provided by their employers. Since immigrants are more likely to work for small firms, this partly explains why so many immigrants and their children are uninsured. In 1998, 33 percent of persons in immigrant households worked for an employer with fewer than 25 employees compared to 25 percent of workers in native households. However, the larger share of workers from immigrant households employed by small firms does not account for the large difference in the rates of insurance coverage for persons in immigrant and native households. Table 10 shows that even after accounting for employer size, full-time workers in immigrant households are much less likely to be insured by their employer and they are also less likely to have insurance from some other source. As already pointed out, 73.5 percent of workers in immigrant households employed by a small firm (fewer than 25 workers) did not have employer-provide health insurance compared to 59.9 percent of workers in native households employed by firms of the same size. Thus, a very sizable gap (13.6 percentage points) remains between full-time workers in immigrant and native households even after employer size is taken into account.
Table 10 also shows that about one-third of the workers in immigrant households employed by a small company who do not have employer-provided health insurance are able to get insurance elsewhere. Of workers in native households working for small employers and who are not insured through their job, more than half were able to obtain health insurance from some other source. This shows that not only are workers in native households more likely to be covered by insurance from their employer, they are also more likely to get insurance from another source when not covered by employer-provided health insurance. This same pattern exists throughout every cell in Table 10.
As already discussed, a greater percentage of adults in immigrant households have few years of schooling. This contributes significantly to the high percentage without insurance (see Table 2). But Table 10 also shows that even controlling for education and employer size, full-time workers in immigrant households are much more likely to be uninsured than workers in native households. This can be seen clearly by looking at college educated workers, who are the most likely to have insurance. In 1998, 31.8 percent of full-time workers in immigrant households with four or more years of college did not have insurance from their employer, compared to 21.9 percent in native households. This nearly 10-percentage-point gap in the rate of employer-provided insurance between college graduates in immigrant and native households narrows somewhat among workers employed by larger companies. Of workers in immigrant households with at least a college education and employed by a firm with between 100 and 499 employees, 23.2 percent did not have insurance through their job. For those in companies with more than 500 employees, 17.4 percent did not have insurance from their employer. For natives the corresponding figures are 16.4 percent and 13.7 percent. Although the differences associated with educated workers in immigrant and native households are somewhat smaller for those employed by larger companies, college-educated workers in native households are still more likely to have employer-provided health insurance than college-educated workers in immigrant households. The same general patterns exist in the rest of the table. Workers in immigrant households are much more likely to be without employer-provided health insurance or health insurance of any kind than their counterparts in native households, even after controlling for education level and employer size.
While the CPS does not ask respondents why they do not have health insurance, it seems plausible that the difference in rates of employer-provided coverage may partly reflect attitudinal differences between immigrants and natives. Since there is often some cost to the employee, a larger percentage of workers in immigrant households may be choosing to keep the employee’s contribution and simply not enrolling in their employers insurance plan. Given the lower average income and education level of immigrant households, this is not surprising. However, immigrants with a college education should have incomes that allow them to purchase insurance, even if their employer makes them pay a large share of the costs. Even if we confine our analysis to only college-educated workers 25 to 64 years of age, employed full-time, in households with income of more than $75,000, we still find that those in immigrant households are about twice as likely as those in native households with the same characteristics to be without insurance.
In addition to not taking advantage of insurance when it is available, lower rates of employer-provided health insurance among immigrant workers may also reflect the fact that immigrants, in contrast to natives, do not think insurance is as important a fringe benefit when choosing where to work. Having come from societies where health insurance is rare, some immigrants may be more willing to work for employers who do not offer health insurance. If this is the case, it would be roughly analogous to the often-made argument that immigrants are willing to work for lower wages than natives. A difference in how they view the value of health insurance might explain why a much higher percentage of college-educated full-time workers in immigrant households do not have employer-provided health insurance.
Further support for this possibility can be found by looking at the percentage of workers by education who have no insurance of any kind. Looking at the most educated workers indicates that 14.5 percent of all full-time workers in immigrant households with at least a college-education did not have health insurance in 1998 (bottom of Table 10). In contrast, only 5.9 percent of college-educated full-time workers with at least a college education in native households were uninsured. Part of the reason for these differences in overall rates of insurance coverage is that a much larger percentage of educated natives who did not get insurance from their employer acquired it from another source. Of college-educated workers in immigrant households who did not have employer-provided health insurance, 56 percent were able to get insurance from another source. In contrast, of college-educated workers in native households who did not have employer-provided health care, 73 percent obtained insurance from another source. This would seem to support the argument that a smaller share of educated persons in immigrant households desire to have insurance than educated persons in native households. Since educated workers generally have the highest incomes and should therefore be able to afford coverage if it is not provided by their employers, this suggests that many immigrants may simply be choosing not to have health insurance, even if they have the financial resources to purchase it on their own.
If a larger percentage of immigrants than natives do not see health insurance as a necessity, there will be a number of negative implications. For the immigrant and his family it may mean a reduction in the amount and quality of the health care they receive. It can also be seen as irresponsible in a society that will provide emergency and some basic health care to all. By not getting insurance when it can be obtained, immigrants are in effect shifting the costs of their health care from themselves to the rest of society, which will be forced to provide more funding for services to the uninsured.
Of course, the decision is about whether to purchase health insurance, where to work, and what fringe benefits are desirable are complex and can be affected by many factors not considered here. While the evidence suggests that immigrants are less likely to want health insurance than natives, other explanations are certainly possible. It should also be recalled that other evidence presented in this study indicates that the primary reason persons in immigrant households are much more likely to lack insurance is their lower level of education and lower incomes. Still, the larger proportion of educated and affluent immigrants without insurance is clearly an important finding. Exploring this question in greater detail should be an area of future research.
Geographic Area
So far this report has only examined health insurance coverage based on the individual characteristics of persons in immigrant and native households at the national level. While certainly important, national figures may obscure important differences that exist across the country. For this reason, we now turn to an examination of insurance coverage by state and metropolitan area. The question of immigration’s impact on the size of the uninsured population at the sub-national level is especially important because state and local governments pay many of the costs associated with providing care to those without insurance.
Insurance Coverage by State
Table 11 provides data on insurance coverage for persons in immigrant and native households for the eight states with the largest number of persons living in immigrant households. In 1998, 76.6 percent of all persons living in immigrant households resided in one of these states. The first and second columns in the table report the percentage of persons in immigrant and native households without health insurance. The last two columns of the table provide the percentage uninsured in each state using a combined sample of the March 1997 and 1998 CPS. The fact that the figures change so little when 1997 data are added demonstrates the strength of the findings in the first two columns. The table indicates that in all eight states, persons in immigrant households are much more likely to be uninsured than are individuals in native households. The differences in rates of insurance coverage for persons in immigrant and native households in 1998 are statistically significant using a 90 percent confidence interval. In light of non-sample errors that exist in any sample, including the CPS, the smaller difference between the two groups in Massachusetts should be interpreted with caution, especially since the state has the smallest population living in immigrant households of those listed in Table 11.
The largest difference between immigrants and natives can be found in Arizona, where persons in immigrant households are almost three times as likely to have no insurance as persons in native households. Arizona is by no means the only state where the difference in insurance coverage is enormous. In Texas, California, New York, and Illinois, persons in immigrant households are more than twice as likely as those in native households to be uninsured. And while persons in immigrant households in Florida and New Jersey households are not twice as likely to be uninsured as those in native households, the difference in both states is very close to being so. Table 11 makes clear that with the possible exception of Massachusetts, lack of health insurance is a serious problem among persons in immigrant households in every major immigrant-receiving state in the country. Low rates of health insurance coverage among immigrants and their children is not simply confined to one state or even one part of the country. While Table 11 shows that the situation is worse in western states, lack of insurance among persons in immigrant households also is a serious problem in New York, Florida, Illinois, and New Jersey. Thus, despite the fact that immigrants differ significantly across states by country of birth and other demographic characteristics, health insurance coverage is a serious problem in immigrant communities throughout the country.
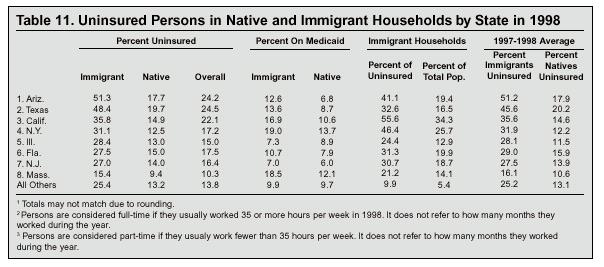
The fourth and fifth columns of Table 11 report the percentage of persons in immigrant households receiving Medicaid. In five of the eight major-immigrant receiving states, persons in immigrant households are much more likely to be on Medicaid than are persons in native households. In the other three states, Medicaid use for persons in immigrant households is roughly equal to that of natives. Since immigrant use of Medicaid is as high as or higher than that of natives in every state, it is clear that lack of access to Medicaid by itself cannot be seen as the reason why individuals living in immigrants households are so much more likely to be without insurance.
Combining the Medicaid use rates with the percentage uninsured indicates that an enormous proportion of immigrants and their children either have no insurance or must have it provided to them at taxpayer expense. For example, 63.9 percent and 62 percent, respectively, of persons in immigrant households in Arizona and Texas are on Medicaid or have no insurance, and more than half of the persons in immigrant households in California and New York also have no insurance or have it provided to them by the government. In the other four states, more than one-third of the population in immigrant households is uninsured or on Medicaid. Massachusetts in particular does not seem to be the "success" story it appears to be when only the percentage of persons in immigrant households without coverage is considered. While immigrant households in Massachusetts do have the highest rate of insurance coverage of any major immigrant receiving state, this fact partly reflects the very heavy use of Medicaid by immigrant households in that state. In 1998, nearly one out of five persons in Massachusetts living in an immigrant households used Medicaid — only New York has a higher rate of Medicaid associated with immigrants.
By itself, the high percentage of persons in immigrant households without insurance would not necessarily create a large burden for the health care system in these states were it not for the fact that so many immigrants have entered the country in the last three decades. If there were relatively few immigrants then a large percentage without health insurance would not necessarily be of concern to the nation as a whole.14 And dealing with the problem would likely be both easier and less costly. In order to measure the impact immigration has on the size of the uninsured population in each state, the sixth column of Table 11 shows the proportion of the entire uninsured population who live in immigrant households. In California, Arizona, and New York, the impact of immigration on the size of the uninsured population is difficult to overstate. In all three states, more than 40 percent of the uninsured live in immigrant households. In the other five states the impact of immigration on the size of the uninsured population is somewhat smaller, but still very large. In Texas, Florida, and New Jersey, immigrant households account for nearly a third of the uninsured and in Illinois, one fourth of the uninsured live in an immigrant households. Even in Massachusetts, one out of five uninsured residents lives in an immigrant household. There can be little doubt that in all of these states, immigration has had a significant effect on the size of the uninsured population. For these states, any discussion of the uninsured problem must include a discussion of immigration policy.
The seventh column in Table 11 shows the percentage of the total population in each state who live in immigrant households. It shows that the immigrant percentage of the uninsured (column six) is not proportional to their representation in the total population. In fact, in some states immigrants represent nearly twice the proportion of the uninsured as they do of the overall population. Further evidence of immigration’s impact on the problem of insurance coverage can be found in the third column of Table 11, which shows the overall percentage of the population in each state who are uninsured. By comparing the percentage of persons in native households who are uninsured (column two) with column three one can see that the presence of immigrants in most states dramatically increases the total share of the states’ populations who are without health insurance. Taken together, the results in Table 11 indicate that in the major immigrant-receiving states, immigration has had a substantial impact on the size of the uninsured population. Health insurance coverage is a significant problem for persons in immigrant households throughout the country. The problem is not confined to one state or even one region. Lack of health insurance among immigrants and their children is a problem national in scope.
Insurance Coverage by Metropolitan Area
In addition to examining insurance coverage by state, it also is possible to examine rates of insurance coverage in the nation’s largest metropolitan areas. Because of the sample size in the CPS, however, immigrant insurance coverage can only be analyzed in a few very large Metropolitan Statistical Areas (MSA). However, it is possible to use combined metropolitan areas, referred to as Consolidated Metropolitan Statistical Areas (CMSA) by the Census Bureau, to examine the impact of immigration at the local level using the March 1998 CPS.
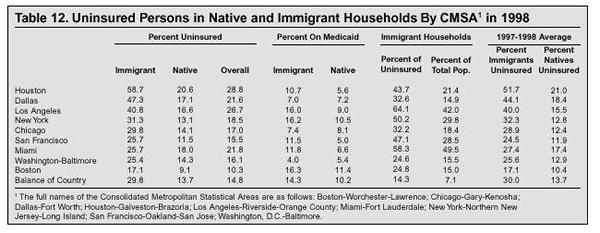
In 1998, there were 18 officially designated CMSAs. Of these, nine have a sufficiently large number of persons living in immigrant households to examine them using the CPS. Table 12 is structured in the same manner as Table 11 except that it reports figures for CMSAs and not states. The table shows that in every CMSA with a large immigrant population, lack of health insurance coverage is dramatically higher among persons in immigrant households than it is for individuals in native households. While the CPS is not designed to measure differences in sub-populations within CMSAs, the difference between the two is statistically significant in every CMSA. The fact that the 1997-98 two-year average in the last column of the table shows very similar differences in rates of insurance coverage lends strong support to the findings in the first two columns of the table. However, the differences between immigrant and native households in Miami and Boston are close enough that non-sampling errors may create statistical insignificance. Therefore, the difference in those two cities should be interpreted with some caution.
Putting aside Miami and Boston, which account for only about 5 percent of the nation’s total population living in immigrant households, the difference between immigrant and native insurance coverage in the nation’s largest cities is enormous. In six of the nine metropolitan areas, persons in immigrant households are more than twice as likely to be without health insurance as persons in native households. While higher than that of natives in every metropolitan area, the percentage of persons in immigrant households without insurance varies significantly between cities. In 1998, It ranged from a high of 58.7 percent for persons in immigrant households living in the Houston CMSA to a low of 17.4 percent for persons in immigrant households in the Boston area. Table 12 also shows that even in metropolitan areas where the immigrant population tends to be more skilled and have higher incomes, such as San Francisco and Washington, a very large percentage of immigrants lack health insurance. The findings in Table 12 confirm the results reported in Table 11 — lack of health insurance among persons in immigrant households is a problem throughout the country.
As a share of the total uninsured population, the highest percentage is found in Los Angeles, where 64.1 percent of all uninsured persons live in immigrant households. Miami is next with 58 percent, and New York is third with 50.2 percent of the uninsured living in immigrant households. The fact that immigrants and their children account for more than half of the uninsured in these cities may not be too surprising given the very high level of immigration to these metropolitan areas in recent decades, although in each city immigrant households are still disproportionately represented among the uninsured. But even in Boston and Washington, cities with much smaller immigrant populations, persons in immigrant households account for almost one-fourth of the uninsured. The figures reported in Table 12 indicate that while the debate over the uninsured may not yet reflect it, in many parts of the country immigration has become a determinate factor in the size of the uninsured population. Without a change in immigration policy, immigrant households will likely account for a growing share of the uninsured in cities like Boston and Washington as well as other parts of the country in the near future.
Tables 11 and 12 show that in many parts of the country, any discussion of the uninsured must include a discussion of immigration policy. In the major immigrant-receiving cities and states, the size of the uninsured population is one-third larger to twice the size it would otherwise be were it not for immigrants and their children. Clearly, to exclude immigration policy from the debate over how to deal with the health care insurance issue would be to ignore a central aspect of the problem.
Policy Implications
The findings in this paper clearly show that immigration policy has significantly increased the size of the uninsured population in the United States. Although they comprise only 13.1 percent of the nation’s total population, persons in immigrant households now account for 26.1 percent of the uninsured. Moreover, recent immigrants and their children account for more than half of the growth in the uninsured population since 1994. Knowing that our immigration policy causes the uninsured population to grow significantly in the United States does not, of course, tell us what we should do about this problem. As already discussed, there are a number of reasons to be very concerned about this growing problem. Assuming that we are concerned about this situation, two sets of policy options would seem to make sense. The first set of changes that might be pursued would be to adopt a new immigration policy that reduces the flow of immigrants who are likely to be end up among the ranks of the uninsured. This would help to ensure that immigration does not continue to add to the health insurance problem in the future. The second set of policy options would involve the development and implementation of policies that address the needs of uninsured immigrants and their children already here. This would have to be done in the context of existing efforts to provide health care and/or insurance coverage to the uninsured and it would have to be designed to meet the specific needs of immigrant families. Let us consider changes in immigration policy first.
Changing Immigration Policy
As we have seen, the lack of insurance coverage among immigrants stems partly from the low levels of education and high poverty rates among immigrants. Because of the limited value of their labor in an economy that increasingly demands educated workers, those with few years of schooling are the most likely to hold jobs that do not have health insurance. Or, if insurance is offered, the employee must pay a large share of the costs. Since workers with few skills also tend to have the lowest incomes, less-skilled workers are among the most likely not to be able to afford coverage when it is not provided by an employer. As a result, there are very large differences in rates of insurance coverage by education. For example, while 19 percent of working-age adults in immigrant households with a college education were found to be uninsured in 1998, 53 percent of high school dropouts in immigrant households were uninsured. Therefore, selecting a larger share of immigrants based on their skills would be very helpful in increasing the percentage of future arrivals who are covered by insurance. In addition, selecting persons with more education, who tend to have higher incomes, increases the ability of immigrants to purchase insurance on their own if it is not provided through their job. Changing the skill profile of newly arrived immigrants would require changes in both the selection criteria for legal immigrants and significantly stepped-up efforts to reduce illegal immigration.
Of course, there are benefits to immigration and these might be enough to offset the costs associated with the dramatic increase in the size of the uninsured population resulting from current immigration. In 1997, the National Research Council (NRC) examined the economic and fiscal effects of immigration on the United States and concluded that the likely economic benefits from immigration were very small relative to the size of the American economy. (Edmonston and Smith, 1997) Moreover, the NRC study found that the economic gains from immigration are the result of lower wages experienced by the least educated and poorest Americans who face the most competition from immigrant workers for low-wage jobs. Even if it does result in slightly higher returns on capital and slightly lower consumer prices, holding the wages of the poorest workers may be viewed by many as a cost rather than a benefit of immigration. The NRC also found that the net drain on public coffers (tax payments minus services used ) from immigrant households is enough at the present time to offset entirely the small positive economic effects that come from holding down the wages of the poor. While opinions on the costs and benefits of immigration differ, the NRC report was prepared by many of the top scholars in the field. It clearly shows that we can curtail immigration without any worry that it will harm the U.S. economy.
Of course, a low level of educational attainment is not the only reason the rate of health insurance coverage associated with immigrants is so low. One of the central findings of this report is that even among more educated and higher income immigrant households, lack of insurance coverage is surprisingly common. The fact that so many persons in immigrant households who should be able to afford coverage do not have it, suggests that many immigrants may simply not see the value of having health insurance. This may reflect the fact that migrants from countries with little or no tradition of health insurance, even the well-educated, retain the cultural attitudes and norms of their homelands. Therefore, it is entirely possible that increasing the size of the uninsured population is an unavoidable consequence of large scale migration from less modern and underdeveloped countries, where having insurance is not the norm. Since relatively few persons from the developed and more affluent parts of the world wish to come to the United States, persons from the less developed parts of the world will continue to comprise the vast majority of new immigrants as long as immigration remains at the current high level. Thus, it may be that a significantly larger uninsured population is simply an unavoidable cost associated with mass immigration. However, this point should not be overstated. It is clear from the data presented in this report that increasing the skill level of newly arriving immigrants would dramatically increase the percentage who obtain insurance. To ensure that a larger proportion of immigrants who enter in the future have the skills to complete in the modern American economy, and acquire health insurance, some changes in immigration policy are clearly warranted. This seems especially reasonable when one considers it is generally assumed that with the exception of refugees, immigration is supposed to benefit the United States. Therefore, it makes perfect sense to alter immigration to serve that end.
Changing Legal Immigration
In most years, 65 to 70 percent of visas are allotted to the family members of U.S. citizens and LPRs. Family relationships could continue to be a central part of immigration policy; however, limiting which relatives are eligible for admission could reduce the number of immigrants admitted without regard to their skills. The Commission on Immigration Reform chaired by the late Barbara Jordan suggested limiting family immigration to the spouses, minor children, and parents of citizens and the spouses and minor children of LPRs. This would eliminate the preferences now in the law for the siblings and adult children (more than 21 years of age) of citizens and Legal Permanent Residents. The preference for the spouses and children of non-citizens should also probably be eliminated, since these provisions apply to family members acquired after the alien has received a green card, but before he has become a citizen.15 If the parents of citizens were also eliminated as a category, family immigration would be lowered to roughly 300,000 per year, and the number would likely fall to 200,000 in a few years.
Humanitarian immigration should also undergo some changes. A greater effort should be made to limit asylum and refugee status to those who are genuinely in need of permanent resettlement because of persecution or a well-founded fear of persecution. The expansion of asylum grounds to groups not originally intended is likely to undermine public support for this small but needed category of admission. Abuse of asylum law also encourages illegal immigration by allowing those who make it into the United States to claim asylum on specious grounds in an effort to forestall deportation. As for refugees, the system must continue to remain flexible and in some years it may need to expand well beyond the 50,000 originally intended by the Refugee Act of 1980. Limiting resettlement to 50,000 would still allow the United States to take in nearly all of the persons identified by the U.N. High Commissioner for Refugees as needing permanent resettlement. At present, refugee policy is highly politicized and many of the refugees admitted to the United States do not meet the U.N.’s definition.
For employment-based immigration, the most important change would be to drop the 10,000 visas for unskilled workers.16 In addition to allowing in unskilled immigrants, this category also encourages illegal immigration because it offers the hope to unskilled illegal aliens that they will find an employer who will eventually petition to bring them in legally. The Jordan Commission also suggested eliminating the visa lottery. While the lottery represents 6 to 8 percent of the legal immigrant flow in most years, it makes little sense to admit immigrants based on luck. It also stimulates further family immigration because the winners can then petition to bring in bothers and sisters, adult children, and parents. Restricting family immigration to only the spouses and minor children of U.S. citizens, rationalizing humanitarian immigration, and ending the lottery would significantly reduce the number of legal immigrants admitted each year without regard to their ability to compete in the U.S. economy. This would help to ensure that immigration does not continue to cause a huge increase in the size of the uninsured population.
Reducing Illegal Immigration
As we have seen, most of the people living in immigrant households without insurance are legal immigrants or the U.S.-born children of immigrants; however, reducing illegal immigration would still be helpful in lowering the number of immigrants entering each year who do not have health insurance. Illegal immigration is undoubtedly the lowest-skilled immigration, with an estimated two-thirds having no health insurance. Among those who study the issue, there is broad agreement that cutting illegal immigrants off from jobs offers the best hope of reducing illegal immigration and, since 1986, it has been unlawful to employ illegal aliens. To date, however, worksite enforcement efforts have been ineffective. Three steps are needed to make worksite enforcement more effective. First, a national, computerized system that allows employers to verify that persons are legally entitled to work in the United States needs to be implemented. Tests of such systems have generally been well received by employers (Bolton, 2000). Second, the Immigration and Nationalization Service must significantly increase worksite enforcement efforts. Congress has repeatedly failed to increase funding for worksite enforcement. Third, more also could be done at the border. Despite increases in funding over the last few years, efforts along the southern border remain grossly inadequate. A real effort to control the border with Mexico would require perhaps 20,000 agents and the development of a system of formidable fences and other barriers along those parts of the border used for illegal crossings.
The cuts in legal immigration proposed earlier would also go a long way toward reducing illegal immigration in the long run because the current system of legal immigration creates a strong incentive to come illegally. There are approximately four million people qualified for immigration to the United States, but who are waiting their turn to receive the limited number of visas available each year in the various family categories. Such a system encourages those who have been selected, but have to wait, to simply come to the United States and settle illegally in anticipation of the day they are granted visas. Eliminating the sibling and adult children categories would alleviate this situation by doing away with the huge waiting lists. In addition to reducing the incentive to come before a green card is issued, cuts in legal immigration would also be very helpful in controlling illegal immigration because communities of recent immigrants serve as magnets for illegal immigration, providing housing, jobs, and entree to America for illegals from the same country. It is no coincidence that the top immigrant-sending countries are also the top countries in sending illegal immigrants to the United States. Sociological research shows that one of the primary factors influencing a person’s decision to emigrate is whether a family member or member of their community has already come to United States (Massey and Espinosa 1997; Palloni, Spittel, and Ceballos 1999). Thus, allowing in large numbers of legal immigrants is one of the leading causes of large-scale illegal immigration.
The changes in legal and illegal immigration policy outlined above would restore immigration levels to their historical average of about 300,000 to 400,000 annually in a few years. Even with these changes, the United States would continue to accept twice the number of immigrants as any other country in the world. More important, by limiting the number of immigrants allowed into the country without regard to their skills, these changes would insure that immigration will not continue to significantly add to the uninsured population in the way that it has in the recent past.
Increasing Insurance Coverage Among Immigrants Already in the Country
While lowering the number of less-skilled legal and illegal immigrants entering each year would ensure that fewer immigrants admitted in the future end up among the ranks of the uninsured, it would not immediately increase the rate of insurance coverage among immigrant households currently residing in the United States. Reducing the size of the uninsured population by changing immigration policy should, over time, free up resources from federal, state, and local governments so they can do more for the uninsured. And this would clearly be a desirable outcome for uninsured immigrants and their children already in the country. This alone, however, will not solve the problem. The most direct and simplest way to provide health insurance to persons in immigrant households would be for the government to provide free health insurance or insurance at greatly reduced cost to all those who do not have it. This strategy has been extremely effective in providing health insurance coverage to the elderly. Because of Medicare, persons over age 65 have the highest rate of insurance coverage of any sub-population in the country. Of course, the primary disadvantage of programs of this kind is the cost. Providing insurance coverage to the 11.6 million people in immigrant households without insurance would be very expensive. Even providing insurance coverage to only the 7.4 million people in immigrant households who live in or near poverty and have no insurance would cost tens of billions of dollars. For example, expenditures on the more than 30 million recipients of Medicaid amounts to more than $150 billion a year. Providing Medicaid coverage to only the 7.4 million persons in immigrant households in or near poverty, to say nothing of the 16.4 million poor and near-poor in native households, might cost taxpayers upwards of $30 billion annually.
Even if providing coverage to all of the uninsured with low-incomes, including those in immigrant households, is thought to be prohibitively expensive, more can be done to increase their rate of insurance coverage. As we have seen, most persons without health insurance live in households where at least one person works. Thus, one set of options that should be pursued would involve making it easier for businesses to cover their employees. This might involve changing regulations and tax policy with the intent of making it less expensive for businesses to provide private health insurance to their workers. Tax credits might also make private insurance more affordable for the working poor and near poor. Both the Republican and Democratic nominees for president have proposed tax credits totaling billions of dollars a year so the working poor can more easily purchase private health insurance. In addition to increasing private insurance coverage, greater efforts on the part of government, at all levels, to provide insurance to those without it could have a significant effect on the rate of insurance coverage among those most likely to be uninsured. So as to contain costs, such efforts could be specifically targeted at subgroups of the uninsured, such as children and those with the lowest incomes. A number of proposals have been made in this regard in recent years and some new initiatives have been implemented by the federal and state governments. The new State Children’s Health Insurance Program or SCHIP, enacted in 1997, is one such effort. By April of 2000, SCHIP had insured an estimated one million children. It is hoped that it will eventually reach an estimated 2.5 million eligible children, at a cost of over $4 billion annually to the federal government when fully implemented. As the SCHIP shows, even providing insurance coverage to a small fraction of the 44.3 million U.S. residents without health insurance will not be cheap. For this reason, changing immigration so that it does not continue to add to the problem clearly makes sense. The SCHIP program also demonstrates how immigration can make reducing the size of the uninsured population vastly more difficult. As already pointed out in the discussion on insurance coverage by age, in just the last four years immigration has increased the number of children under the age of 19 (SCHIP’s target population) without insurance by more than 700,000 — enough to offset most of the gains made so far under SCHIP.
In addition to making private and government-provided insurance more available, new efforts might be undertaken to educate new immigrants about the need for health insurance. It is clear from the research presented in this report that lack of insurance for persons in immigrant households is not simply caused by the low levels of education and high poverty rates associated with immigrants. Well-educated and high-income immigrant households also are much more likely to be without insurance than similarly situated natives. For example, nearly one in five persons in immigrant households with incomes of more than $50,000 a year were uninsured in 1998. It is very unlikely that programs designed to insure persons with limited incomes would or even should cover most of these individuals. Instead, these individuals should be taking advantage of employer-provided health insurance when it is offered or purchase it on their own if it is not. While it may be seen as paternalistic, efforts to better inform immigrants of the value of health insurance may be helpful in increasing their rate of insurance coverage. This can be justified because, in a society such as ours that will provide at least basic care to all including the uninsured, there is clearly a public interest in increasing the percentage of the population who have health insurance.
Another area where new initiatives may be possible is job retraining. Since the low skill level associated with immigrants is one of the primary reasons so many work at jobs that pay poverty level wages and do not have health insurance, increasing the ability of immigrants to compete in the labor market by improving their job skills is very likely to increase their rate of insurance coverage. Specific programs designed to increase immigrant familiarity with their new country might help to improve their level of insurance coverage. This may include adult education programs designed to increase knowledge of English, the U.S. job market, employee benefit packages, and services available from government and private sources.
Conclusion
For reasons outlined at the outset of this report, the lack of insurance among immigrants and their children is clearly a serious problem. With more than 35 million people living in immigrant households, how immigrants and their children do in the United States should be a matter of concern for anyone interested in the future of our republic. The huge number of persons in immigrants households without health insurance cannot be neglected indefinitely.
Why Has the Problem Been Ignored?
Part of the reason policymakers and researchers interested in health insurance coverage have not devoted much attention to immigration’s role in this growing problem is that they have generally been focused on other issues such as medical inflation, changing employment practices, and Medicaid eligibility. In addition, until recently it was very difficult to estimate the impact of immigration on the size of the uninsured population in United States. Only in 1994 did the Census Bureau begin to ask a nativity question on a regular basis as part of the CPS. Moreover, immigrants are not politically powerful. Many are not citizens and therefore cannot vote or make campaign contributions. Thus, politicians could ignore immigrants without paying much of a political price. Also, as has already been pointed out, immigration is a discretionary policy of federal government. Elected officials in Washington may be reluctant to deal with the problem because to do so would call attention to the fact that a conscious policy that they have either supported or at least not tried to modify has led to an enormous growth in the uninsured population. It is far easier to emphasize the positive effects of current immigration policy and espouse vague platitudes about "a nation of immigrants" than to deal with the problems federal immigration policy creates.
Another important reason the problem has not received the attention it should stems from the nature of the immigration debate. Most of the advocates for immigrants are also advocates for the current high level of immigration. These advocacy groups cannot call too much attention to the fact that immigration is responsible for a large share of the growth in the uninsured population because to do so would highlight a fundamental problem with the very policy they work so hard to keep in place. Thus, those who might be expected to push for greater efforts to help immigrants remain mostly silent on this issue. Costly new programs designed to provide health coverage to immigrants and increase the skills of immigrants so they can better compete in the labor market would undermine one of the arguments most often made by the advocates of high immigration, namely that it is an economic and fiscal benefit to the country. Therefore, in a very real sense, there is a conflict of interest between being an advocate for immigrants and at the same time being an advocate of mass immigration. Supporters of high immigration are trapped by their own rhetoric. As a result, relatively little attention is paid to the millions of immigrants and their children without adequate health care.
A Problem that Cannot Be Ignored.
While some may be tempted to ignore the lack of health insurance among immigrants and their children at a time of relative prosperity, this seems very unwise. In just the last four years immigration has increased the size of the uninsured population by 2.7 million people. Without a change in immigration policy and greater efforts to increase health care coverage among immigrants and their children already in the country, the problem will grow much worse. This can only make it more difficult and costly to solve. The implications of this situation for the immigrants themselves, their children, the health care system, and society as a whole are such that we simply must confront this problem head on. It is our hope that this study will give policymakers, researchers, and all those concerned about the uninsured a better understanding of the central role that immigration policy has played in this problem.
End Notes
1 There is some debate over what exactly the CPS and other date sources measure concerning the duration of being without health insurance. For a discussion of the various data sources that measure the uninsured and their advantages and disadvantages, see Lewis, Ellwood, and Czajka (1998); and Graham and Smith (1995).
2 Includes persons using the Indian Health Service and state programs, such as Medi-Cal.
3 The federal government provides some funding through disproportionate share hospitals (DSH) payments to hospitals that provide care to a large number of uninsured persons. In addition, the federal government provides money to federally qualified health centers (FQHCs) many of whose patients have no insurance. State and local governments also are significant funders of public hospitals and clinics, some of which are FQHCs. In addition, expenditures on the uninsured are made by public health departments, schools, and a variety of state and local entities and programs. For a detailed discussion of taxpayer provided funding for the uninsured, as well as other funding sources, see Lewin and Altman (2000) www.nap.edu.
4 The immigrant population in the CPS includes some illegal aliens and a small number of persons on temporary visas, such as students, which allow them to stay for multiple years in the United States.
5 This figure is for all persons 18 and over who lack a high school education.
6 These figures are based on the March 1996 CPS.
7 The Census Bureau assigns Medicaid coverage to those who are generally regarded as "categorically eligible" based on other characteristics. For example, persons who receive benefits such as public assistance payments are assumed to be covered by Medicaid, even if they do not report such coverage. The same is true for others who are automatically enrolled in Medicare based on age and receipt of Social Security.
8 This estimate is derived by first linking the U.S.-born children of immigrants with their parents’ records. Using the year of arrival information for their parents as well as the individual children’s ages, it is then possible to calculate the number of children born to newly arrived immigrants over this time period.
9 Additional information provided by Dr. Jeffrey Passel of the Urban Institute in personal communication July 12 1999.
10 "Near poverty" is defined as having an income equal to or below 200 percent of poverty line.
11 Household income is based on the same definition as households used throughout this report. Therefore, the numbers presented here do not exactly match those published by the Census Bureau. Please see the Methods and Data section for a complete discussion of how household is defined.
12 Household is defined here in the same manner as it is in the entire report.
13 This figure is for all workers (full- and part-time) 15 years of age and older.
14 Of course the situation for individual immigrant families would still have to be addressed.
15 There is currently a large backlog of persons waiting to enter in the spouses and minor children of LPRs category. A significant portion of these individuals are the family members of IRCA amnesty beneficiaries. It seems unwise to continue to separate these families. Therefore, it would make sense to grandfather in those already on the waiting list. However, no future applications would be taken for the spouses and minor children of LPRs.
16 In 1997, unskilled employment-based immigration was temporally lowered to 5,000 to offset the amnesty given to some illegal aliens from Central America. It will remain at this level until all those eligible have adjusted to legal status.
References
Bolton, Nancy. 2000. Employment Verification Program Survey. Forthcoming. Washington DC: Center for Immigration Studies Report.
Borjas, George. 1999. Heaven’s Door: Immigration Policy and The American Economy. Princeton N.J.: Princeton University Press.
Budetti, John, Lisa Duchon, Cathy Schoen, and Janet Shikles. 1999. "Can’t Afford to Get Sick: A Reality for Millions of Working Americans." The Commonwealth Fund 1999 National Survey of Workers’ Health Insurance.
Campbell, Jennifer. 1999. October. Health Insurance Coverage: 1998. Current Population Reports P60-208. U.S. Census Bureau.
Castro, Janice. 1994. The American Way of Health. Boston: Little Brown.
Clark, Rebecca L., and Jeffrey Passel. 1998. Identifying Legal and Illegal Immigrants in the Census and Current Population Surveys: A New Technique Based on the Occupational Distribution of Illegal Aliens. Washington D.C.: Urban Institute.
Edmonston, Barry, and James Smith Ed. 1997. The New Americans: Economic, Demographic, and Fiscal Effects of Immigration Washington D.C.: National Academy Press.
Fronstin, Paul. 1998. December. "Sources of Health Insurance and Characteristics of the Uninsured: Analysis of the March 1998 Current Population Survey." Employee Benefit Research Institute. Issue Brief No. 204.
Gage, Larry S., and Marsha Regenstein. 1999. "Bolstering the Safety Net." Health Affairs. Vol. 18, No. 5, September/October, 254-257.
Graham, Loftin, and Madeleine Smith. 1995. November. Health Insurance Explaining Difference in Counts of the Uninsured. CRS Report for Congress, Congressional Research Service, November.
Health Policy Consensus Group. 1999. A Vision for Reform: Consumer-Driven Health Care Reform. Washington, D.C.: Galen Institute.
Holahan, John, and Niall Brennan. 2000. March. Who Are the Adult Uninsured. Washington D.C.: Urban Institute. Series B No. B-14.
Lewin, Marion E., and Stuart Altman, eds. 2000. America's Health Care Safety Net: Intact but Endangered. Institute of Medicine. Washington, D.C.: National Academy Press.
Lewis, Kimball, Marilyn Ellwood, and John L. Czajka. 1998. July. Counting the Uninsured: A Review of the Literature. Occasional Paper Number 8. Washington D.C.: Urban Institute.
Massey, Douglas S., and Kristin E. Espinosa. 1997. "What’s Driving Mexico-U.S. Migration? A Theoretical, Empirical, and Policy Analysis." American Journal of Sociology. 102: 4, 939-999.
Mitchell, Alison. 2000. April 12. "Bush is Proposing a Health Plan to Aid the Needy." The New York Times. Page A1.
Morrisey, Michael A. 1996. December. "Hospital Cost Shifting: a Continuing Debate." Employee Benefit Research Institute. Issue Brief No.180.
Morse, Ann. 2000. ASCHIP and Access for Children in Immigrant Families.@ Washington D.C.: National Conference of State Legislatures.
Palloni, Alberto, Mike Spittel and Miguel Ceballos. 1999. Using Kin Data to Falsify Social Networking Hypotheses in Migration. Paper presented at the annual meeting of the Population Association of America.
Sachs, Susan. 2000. January 3. "More Screening of Immigrants for TB Sought." The New York Times. A1.
Styring, William, III, and Donald K. Jonas. 1999. Health Care 2020: The Coming Collapse of Employer-Provided Health Care. Indianapolis, Ind.: Hudson Institute.
Statistical Yearbook of the Immigration and Naturalization Service 1997. U.S. Immigration and Naturalization Service. Washington, D.C.: U.S. Government Printing Office.
Vaughan, Jessica. 1997. Summer. "Laundering Their Status: One-Fourth of 1996 Immigrants are Former Illegals." Immigration Review. Washington D.C.: Center for Immigration Studies. No 29.
Warren, Robert. 1999. Unauthorized Immigrants Residing in the United States: Estimating the Populations, Componets of Change, and Trends, by Broad Area of Origin, 1987 to 1997. Paper presented at the annual meeting of the Population Association of America.